Baghdad College of Medicine / 4
th
grade
Student’s Name :
Dr. Muayed Abbas
Lec. 7
ADRENAL GLANDS &
PARA THYROID
GLANDS
Mon. 14 / 3 / 2016
DONE BY : Ali Kareem
مكتب اشور
لالستنساخ
2015 – 2016
Adrenal Glands Dr. Muayed Abbas
14-3-2016
2
©Ali Kareem 2015-2016
Adrenal Glands & Para Thyroid Glands
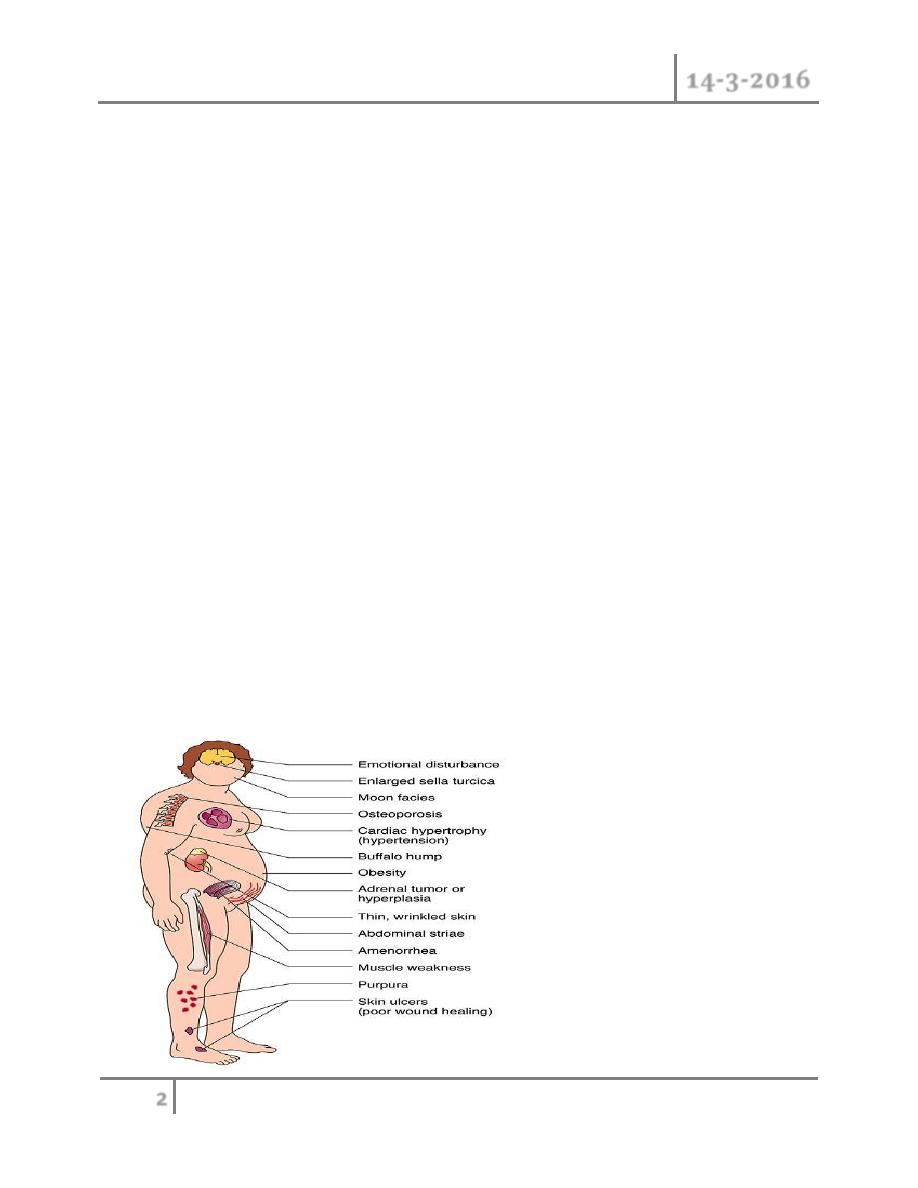
Cushing’s syndrome
o Hypersecretion of cortisol caused by endogenous production of
corticosteroids is known as Cushing’s syndrome.
o It can be either ACTH-dependent or ACTH-independent in origin.
o 85 per cent of ACTH-dependent Cushing’s syndrome :
o Pituitary adenoma that secretes an excessive amount of ACTH(CUSHING
DISEASE)
o Ectopic ACTH-producing tumours (small cell lung cancer, foregut
carcinoid)
o CRH-producing tumours (medullary thyroid carcinoma, neuroendocrine
pancreatic tumour)
o 15 per cent of patients, an ACTH-independent Cushing’s syndrome (low
ACTH levels) is caused by a
o unilateral adrenocortical adenoma.
o Adrenocortical carcinoma
o bilat- eral macronodular or micronodular hyperplasia represent rare causes
of hypercortisolism.
Clinical
symptoms

Adrenal Glands Dr. Muayed Abbas
14-3-2016
3
©Ali Kareem 2015-2016
Diagnosis
o Morning and midnight plasma cortisol levels are elevated, possibly with loss
of diurnal rhythm.
o Dexamethasone fails to suppress 24-hour urinary cortisol excretion.
o Serum ACTH levels discriminate ACTH-dependent from ACTH-independent
disease.
o Elevated or normal ACTH levels provide evidence for an ACTH-producing
pituitary tumour (85 per cent) or ectopic ACTH production. Therefore, in
patients with elevated ACTH,
o MRI of the pituitary gland must be performed. If MRI is negative and
additional venous sampling from the inferior petrosal sinus has excluded a
pituitary microadenoma, A CT scan of the chest and abdomen is warranted
to detect an ectopic ACTH- producing tumour.
o In patients with suppressed ACTH levels, a CT or MRI scan is performed to
assess the adrenal glands.
o Subclinical Cushing’s syndrome is diagnosed if clinical symp toms are
absent in the face of abnormal cortisol secretion.
Treatment
o Medical therapy with metyrapone or ketoconazole reduces steroid synthesis
and secretion and can be used to prepare patients with severe
hypercortisolism preoperatively or if surgery is not possible.
o ACTH-producing pituitary tumours are treated by transsphenoidal resection
or radiotherapy.
o If an ectopic ACTH source is localised, resection will correct
hypercortisolism.
o A unilateral adenoma is treated by adrenalectomy.
o In cases of bilateral ACTH-independent disease bilat- eral adrenalectomy is
the primary treatment.
o Patients with an ectopic ACTH-dependent Cushing’s syndrome and an
irresectable or unlocalised primary tumour should be considered for
bilateral adrenalectomy as this controls hormone excess.

Adrenal Glands Dr. Muayed Abbas
14-3-2016
4
©Ali Kareem 2015-2016
o Subclinical Cushing’s syndrome caused by unilateral adenoma is treated by
unilateral adrenalectomy.
Preoperative management
o
Patients with Cushing’s syndrome are at an increased risk of hospital-
acquired infection, thromboembolic and myocardial complications.
o Therefore, prophylactic anticoagulation and the use of prophylactic
antibiotics are essential.
o Cushing-associated diseases (diabetes, hypertension) must be controlled by
medical therapy preoperatively.
Postoperative management
o After unilateral adrenalectomy supplemental cortisol should be given
postoperatively because the contralateral gland will be suppressed.
o In total, 15 mg/hour is required parenterally for the first 12 hours followed
by a daily dose of 100 mg for 3 days, which is gradually reduced thereafter.
o After unilateral adrenalectomy, the contralateral suppressed gland needs up
to one year to recover adequate function.
o In 10 per cent of patients with Cushing’s disease who undergo a bilateral
adrenalectomy after failed pituitary surgery, the pituitary adenoma causes
Nelson’s syndrome due to continued ACTH secretion at high levels, causing
hyperpigmentation as a result of chemical synergies between ACTH and
melanocyte-stimulating hormone
Primary hyperaldosteronism – Conn’s syndrome
o Defined by hypertension, as a result of hypersecretion of aldosterone
o Patients with hypertension the incidence of PHA is approximately 2 per
cent.
PATHOLOGY
o The most frequent cause of PHA with hypokalaemia is a unilateral
adrenocortical adenoma .

Adrenal Glands Dr. Muayed Abbas
14-3-2016
5
©Ali Kareem 2015-2016
o In 20–40 per cent of cases, bilateral micronodular hyperplasia is present.
o Rare causes of PHA are bilateral macronodular hyperplasia,
glucocorticoid- suppressible hyperaldosteronism or adrenocortical
carcinoma.
Clinical features
o 30 and 50 years of age
o Female predominance
o Hypertension
o Non-specific symptoms: headache, muscle weakness, cramps, intermittent
paralysis, polyuria, polydypsia and nocturia.
Diagnosis
o Assessment of potassium level and the aldosterone to plasma renin activity
ratio.
o MRI or CT should be performed to distinguish unilateral from bilateral
disease.
o MRI or CT should be performed to distinguish unilateral from bilateral
disease.
o Micronodular changes and small adenomas are often underdiagnosed.
o Selective adrenal vein cath- eterisation can help before a decision on non-
surgical or surgical treatment is made
o During selective adrenal vein catheterisation, samples are obtained from the
vena cava and from both adrenal veins and the aldosterone to cortisol ratio
(ACR) is determined in each sample. A significant difference in the ACR
ratio on one side indicates unilateral disease.
Treatment
o The first-line therapy for PHA with bilateral hyperplasia is medi- cal
treatment with spironolactone. In most cases supplemental antihypertensive
medication is necessary.
o Unilateral laparoscopic adrenalectomy is an effective therapy in patients
with clear evidence of unilateral or asymmetrical bilateral disease

Adrenal Glands Dr. Muayed Abbas
14-3-2016
6
©Ali Kareem 2015-2016
o
A subtotal resection can be considered in the case of a typical single Conn’s
adenoma.
PARATHYROID GLAND
o PTH activates osteoclasts to resorb bone, and increases calcium
reabsorption from urine and renal activation of vitamin D with subsequent
increased gut absorption of calcium. Renal excretion of phosphate is also
increased.
Primary hyperparathyroidism
o Primary hyperparathyroidism is commonly a sporadic rather than familial
condition associated with hypercalcaemia and inappropriately raised serum
PTH levels due to enlargement of one or more glands and hypersecretion of
PTH.
Epidemiology
o The prevalence of sporadic primary hyperparathyroidism increases with age
and affects women more than men.
o Familial hyperparathyroidism occurs as part of the following genetically
determined conditions:
o
MEN1 (multiple endocrine neoplasia type 1: Werner’s syndrome);
o MEN2A (Sipple syndrome), rarely in MEN2B; Familial
hyperparathyroidism
Pathology
o The majority (85 per cent) of patients with sporadic primary
hyperparathyroidism have a single adenoma,
o approximately 13 per cent have hyperplasia affecting all four glands and
about

Adrenal Glands Dr. Muayed Abbas
14-3-2016
7
©Ali Kareem 2015-2016
o 1 per cent will have more than one adenoma or a carcinoma.
o In familial disease, multiple gland enlargement is usual.
o A single enlarged gland with three small normal glands is characteristic of a
single adenoma regardless of the histology which may show considerable
overlap between a hyperplastic and adenomatous gland.
o Multiple adenomas occur more frequently in older patients.
o Parathyroid hyperplasia by definition affects all four glands.
o Parathyroid carcinomas are large tumours and typically much more
adherent or even frankly invasive than large adenomas.
o Histology demonstrates a florid desmoplastic reaction with dense fibrosis
and capsular and vascular invasion.
Clinical presentation
o
The classic quartet of ‘stones, bones, abdominal groans and psychic moans’
is rarely observed in developed countries when the diagnosis is usually
detected on serum calcium estimation well before the full picture of severe
bone disease (von Recklinghausen’s disease), renal calculi and calcinosis,
pancreatitis and psychiatric disorder.
Diagnosis
o Although ionised calcium is the physiologically active circu lating element,
total serum calcium is a satisfactory measure.
o The effect of binding to serum proteins must be corrected by upward or
downward correction to a serum albumin level of 40 g/L.
o Inappropriate, i.e. elevated or normal PTH levels in the presence of high
serum calcium is diagnostic of primary HPT.
o Hypophosphataemia and elevated urine calcium excretion are
confirmatory.
o Other causes of hypercalcaemia must be considered and excluded
o Advanced malignancy is the most common cause of hypercalcaemia in
hospitalised patients, due to parathyroid hormone-related peptide (PTHrP)
or bone metastases. The PTH level is suppressed.
Adrenal Glands Dr. Muayed Abbas
14-3-2016
8
©Ali Kareem 2015-2016
o Familial hypocalciuric hypercalcaemia is an autosomal domi nant disorder
characterised by mild elevation of calcium and PTH levels secondary to a
missense mutation in the cell membrane calcium receptor.
o The low urinary excretion of calcium will discriminate this from HPT.
Parathyroidectomy is not required.
Treatment of primary hyperparathyroidism
o At present surgery is the only curative option and should be offered to all
patients with significant hypercalcaemia provided they are otherwise fit for
the procedure.
o There are a number of medical strategies and therapies, particularly in mild
hyperparathyroidism, which include simple expectant treatment until the
calcium level or symptoms reach a level at which surgery becomes more
attractive, low calcium diet, withdrawal of drugs (diuretics and lithium)
which aggravate hypercalcaemia and, more recently, calcium reducing
agents such as bisphosphanates and the calcium receptor agonist cinacalcet.
o Occasionally, patients present with a parathyroid crisis and severe
hypercalcaemia (serum calcium greater than 3.5 mmol/L).
o This results in confusion, nausea, abdominal pain, cardiac arrhythmias and
hypotension with acute renal failure.
o Intravenous saline and bisphosphonate therapy (pamidronate) are required
to correct the dehydration and hypercalcaemia.
o This is best done in a high-dependency unit or even intensive therapy unit
setting to monitor the major physiological fluxes which result.
Indications for operation
o Indications for parathyroidectomy in primary hyperparathyroidism.
o Urinary tract calculi.
o Reduced bone density.
o High serum calciuma.
o All in younger age group <50 years.
o Deteriorating renal function
o Symptomatic hypercalcaemia .

Adrenal Glands Dr. Muayed Abbas
14-3-2016
9
©Ali Kareem 2015-2016
Preoperative localization
o High frequency neck ultrasound is non-invasive and should identify 75 per
cent of enlarged glands. It gives better resolution but reduced penetration
and cannot visualise the mediastinum Nodular thyroid disease is a
confounding factor.
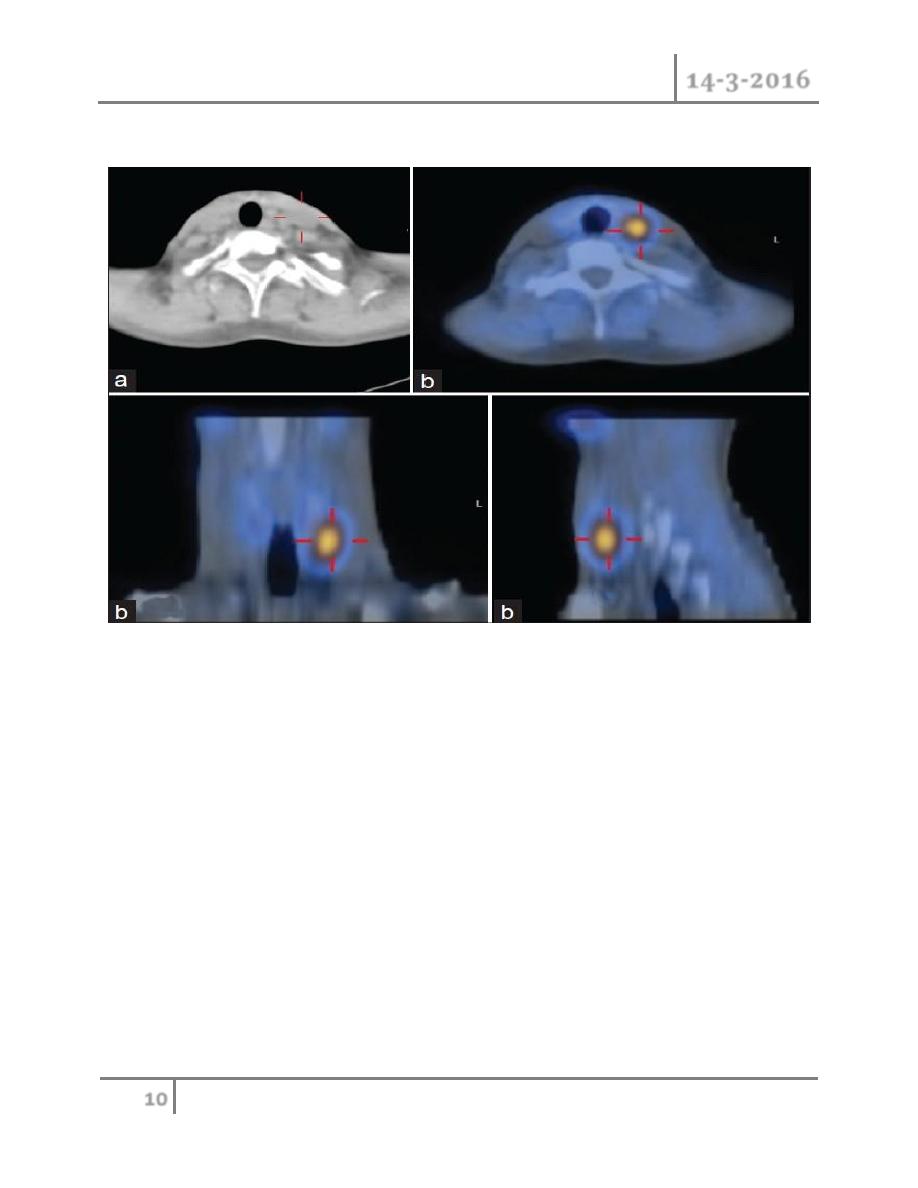
o Technetium-99m (99mTc)-labelled sestamibi (MIBI) isotope scans (also
identify 75 per cent of abnormal parathyroid glands. The area scanned must
include the mediastinum to detect ectopic glands
Technetium-99m (99mTc)-labelled sestamibi (MIBI) isotope scans
• Single-photon emission computed tomography (SPECT) gives a three-
dimensional image which may influence the surgical approach.
• Concordance between ultrasound and sestamibi scan permits a targeted
approach with confidence.
• However, the size of the adenoma is important and imaging and
concordance decline with glands weighing less than 500 mg.
Adrenal Glands Dr. Muayed Abbas
14-3-2016
10
©Ali Kareem 2015-2016
SPECT
Consent for surgery
Preoperative discussion must include the possibilities of:
o Persistent hyperparathyroidism (5 per cent);
o Recurrent laryngeal nerve injury (1 per cent);
o Postoperative haemorrhage (1 per cent);
o Permanent hypoparathyroidism;
o Recurrent hyperparathyroidism.
Operation for primary hyperparathyroidism
o Targeted small incision approach and
o bilateral exploration using a conventional ‘thyroidectomy’ incision are the
most frequently performed.

Adrenal Glands Dr. Muayed Abbas
14-3-2016
11
©Ali Kareem 2015-2016
o Video-assisted (in which a video endoscope is used to reduce the size of
incision and permit bilateral exploration) and totally endoscopic techniques
with multiple punctures have not achieved much popularity.
o Methylene blue infusion to assist in gland identification has largely been
abandoned
o A gamma probe can be used to guide exploration following preoperative
injection of technetium-labelled sestamibi.
o The short serum half-life of PTH means that intraoperative measurement
can be used to confirm that the source of excess PTH production has been
excised.
o Serum levels of PTH are measured pre-incision, pre-removal, 5 minutes
after removal and 10 minutes after removal.
o The assay takes 30 minutes and if the percentage drop is not >50 per cent
then further exploration is indicated.
Operation for primary hyperparathyroidism
o Targeted approach
o Confident preoperative localisation permits a 2–3 cm incision located over
the site of the adenoma
o Conventional approach
o The glands are identified in a systematic manner commencing with the
common sites and working sequentially through to the rare locations.
o All abnormal glands are excised and, in the event of sporadic four-gland
disease, subtotal parathyroidectomy is carried out, preserving
approximately 50 mg of one gland.
o This must be marked with a non-absorbable suture to facilitate any possible
future re-exploration.
o In patients with four-gland disease, transcervical thymectomy is
recommended to reduce the risk of persistent or recurrent
hyperparathyroidism.
o In patients with MEN-1, total parathyroidectomy reduces the risk of
recurrence.
o Preoperative imaging will identify the 1 per cent of patients with a
mediastinal adenoma and allow a single curative operation .

Adrenal Glands Dr. Muayed Abbas
14-3-2016
12
©Ali Kareem 2015-2016
Parathyroid carcinoma
o Cancer of the parathyroid is rare accounting for 1 per cent of cases of
hyperparathyroidism.
o Typical features are very high calcium and PTH levels often with a palpable
neck swelling or occasionally lymphadenopathy.
o Scanning may support the diagnosis.
o The diagnosis is rarely known at the time of exploration but, if suspected,
operation should include excision of the tumour mass with en bloc thyroid
lobectomy and node dissection when indicated.
o The diagnosis is difficult to make histologically and may only become
apparent when recurrent disease presents with hypercalcaemia, increased
serum PTH and evidence of local recurrence.
o Adjuvant or palliative radiotherapy may be indicated and overall survival as
in most endocrine can cers is reasonable with 85 per cent five-year survival.
Management of postoperative hypocalcaemia
o Check serum calcium within 24 hours of total thyroidectomy or earlier if
symptomatic
o Medical emergency if the level is <1.90 mmol/L: correct with 10 mL of 10
per cent calcium gluconate intravenously; 10 mL of 10 per cent magnesium
sulphate intravenously may also be required
o Give 1 g of oral calcium three or four times daily
o Give 1–3 μg daily of oral 1-alpha-vitamin D if necessary
END OF THIS LECTURE…