Glomerulonephritis
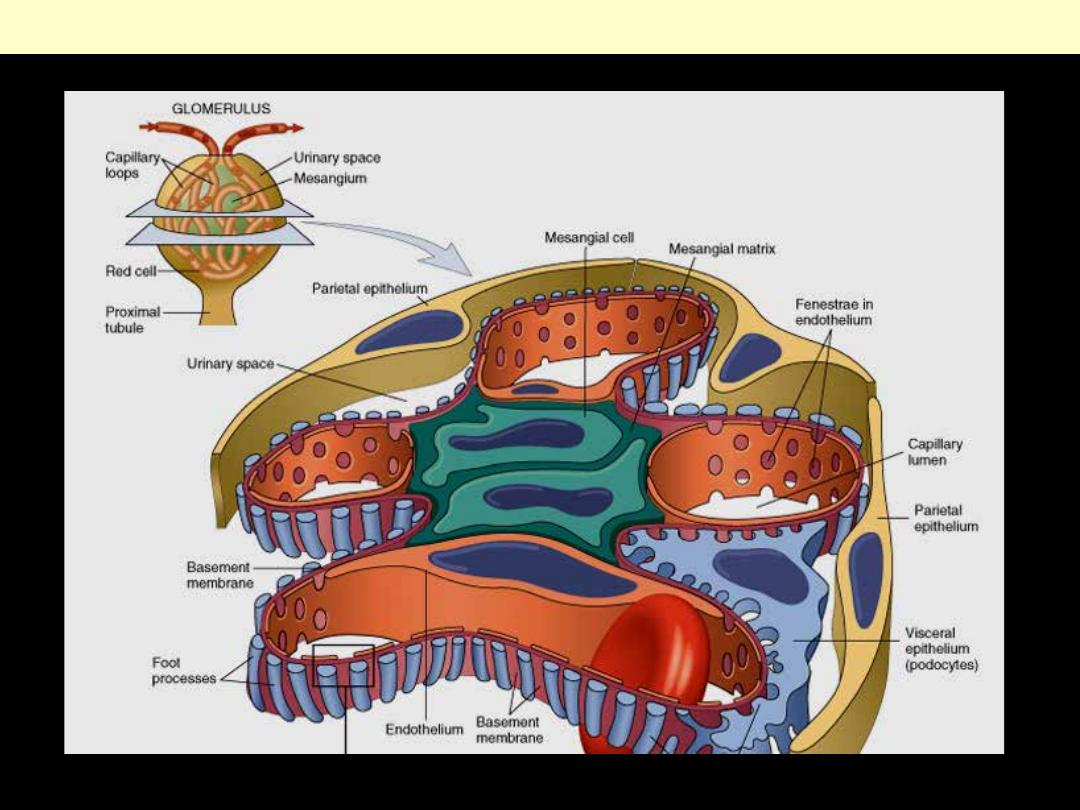
Schematic diagram of a lobe of a normal glomerulus.
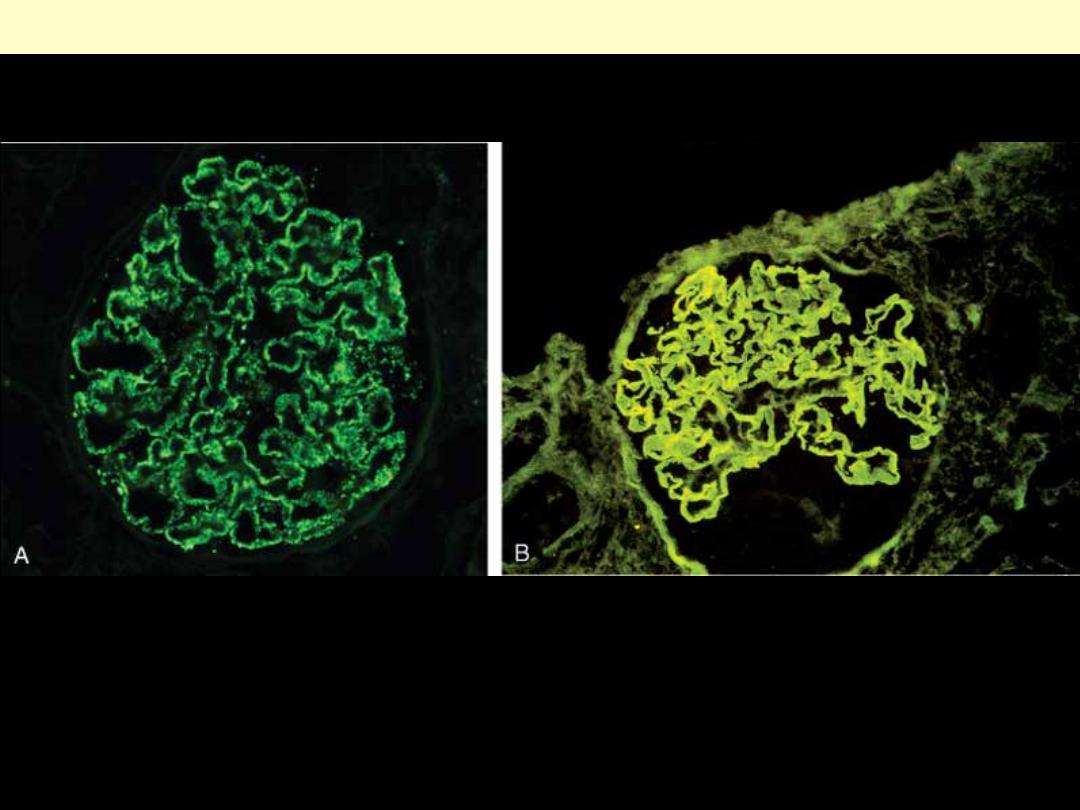
Two patterns of deposition of immune complexes as seen by immunofluorescence microscopy. A,
Granular, characteristic of circulating and in situ immune complex deposition. B, Linear, characteristic
of classic anti-GBM antibody GN.
Deposition of immune complexes as seen by immunofluorescence
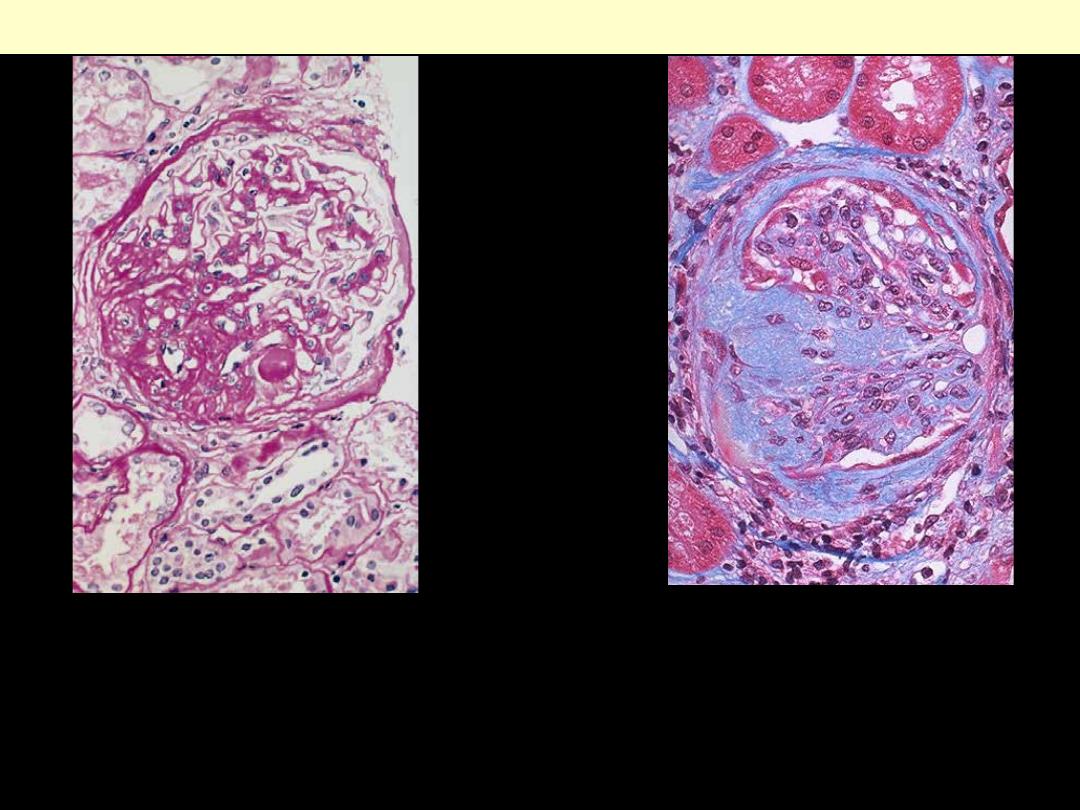
High-power view of focal and segmental
glomerulosclerosis (PAS stain), seen as a
mass of scarred, obliterated capillary
lumens with accumulations of matrix
material, that has replaced a portion of the
glomerulus.
FSGS
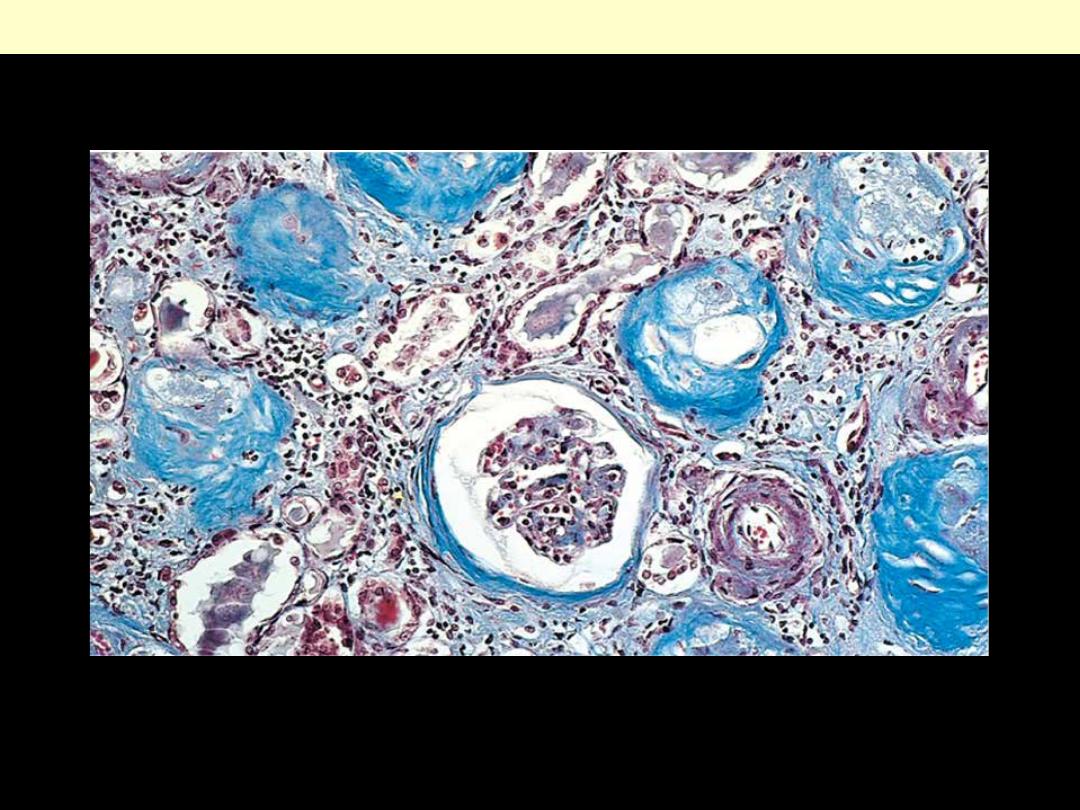
This trichrome stain of a glomerulus in a
patient with FSGS demonstrates blue
collagen deposition. FSGS accounts for about
a sixth of cases of nephrotic syndrome in
adults and children.
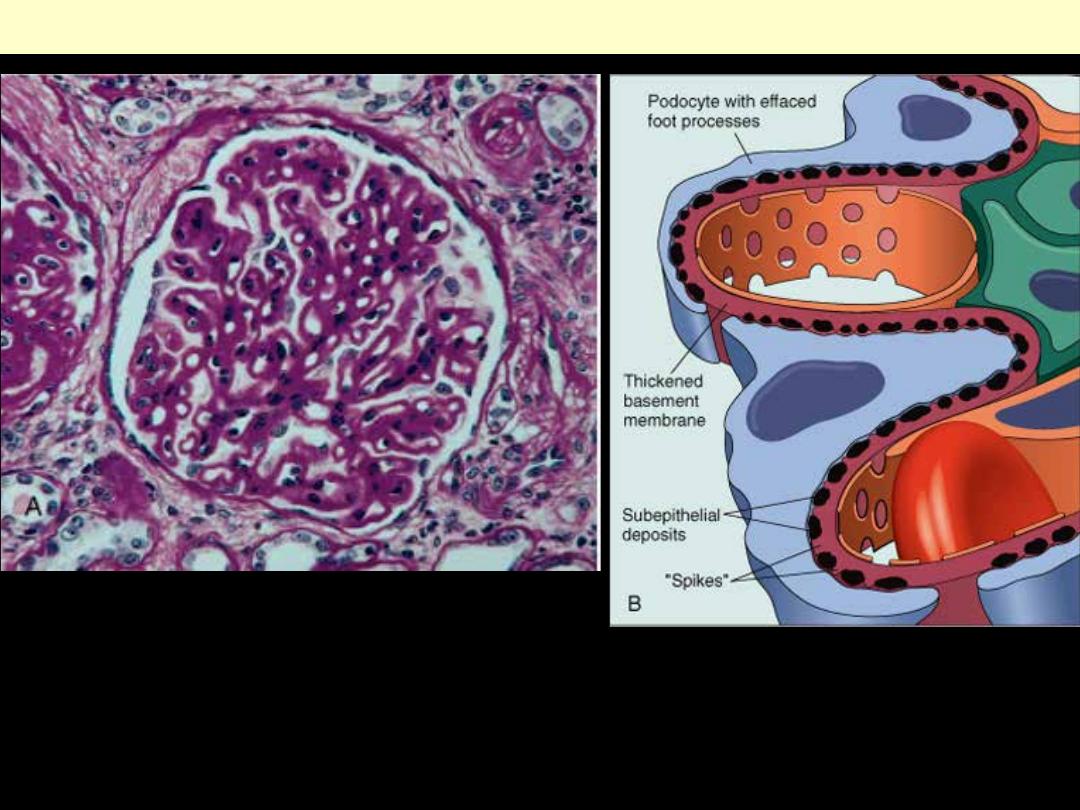
A, Diffuse thickening of the glomerular basement membrane. B, Schematic diagram illustrating
subepithelial deposits, effacement of foot processes, and the presence of "spikes" of basement
membrane material between the immune deposits.
Membranous nephropathy
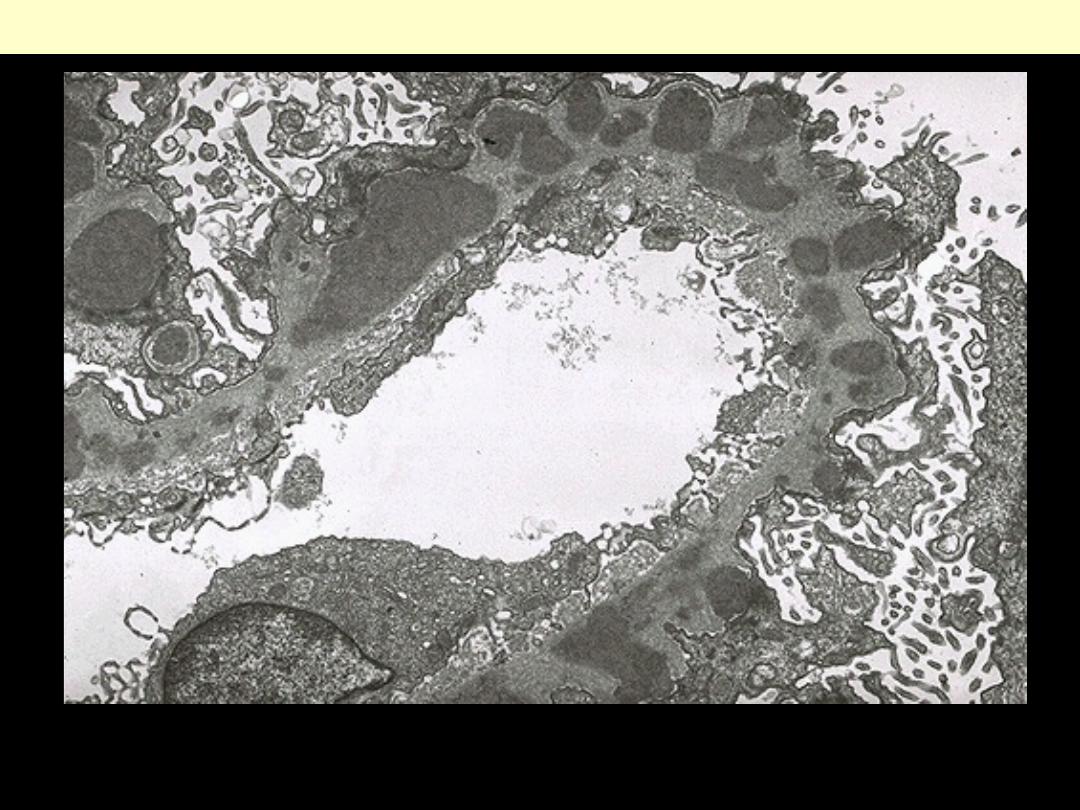
By electron microscopy in membranous glomerulonephritis, the darker electron dense sub-
epithelial immune deposits are separated by an intervening small, spike-like protrusions of
GBM
Membranous nephropathy
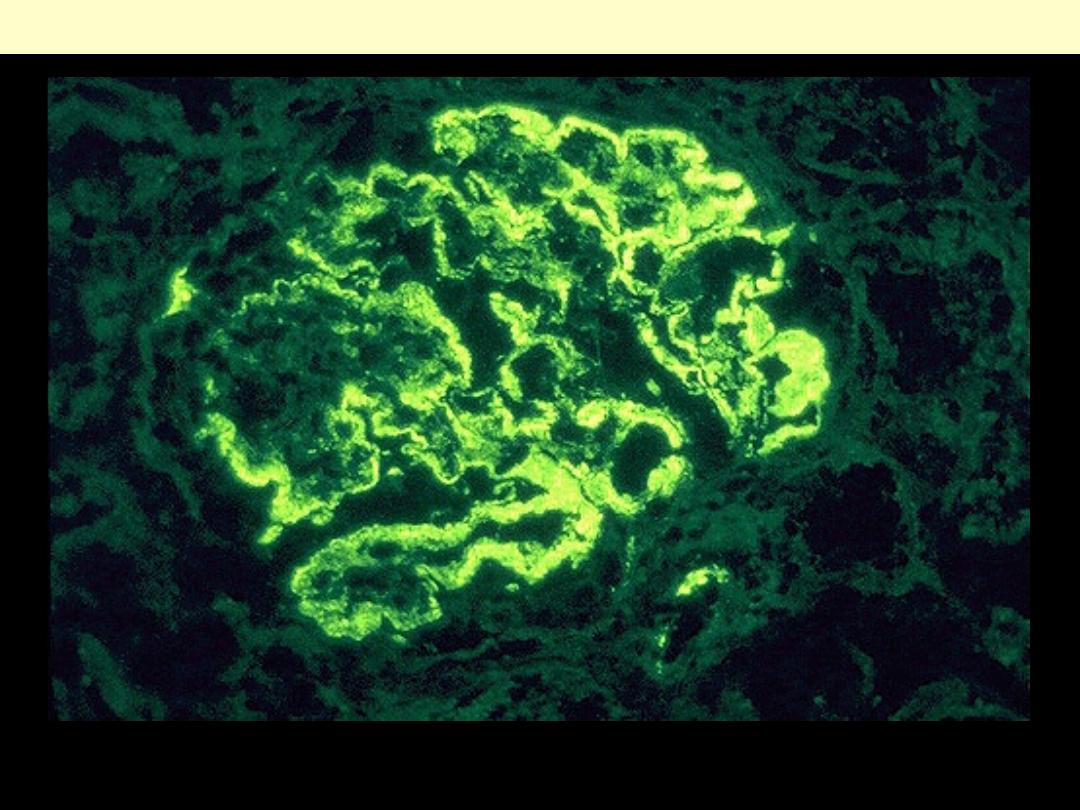
Membranous glomerulonephritis is an immunologically mediated disease in which
peripheral and granular deposits of mainly IgG and complement collect in the basement
membrane
Membranous nephropathy
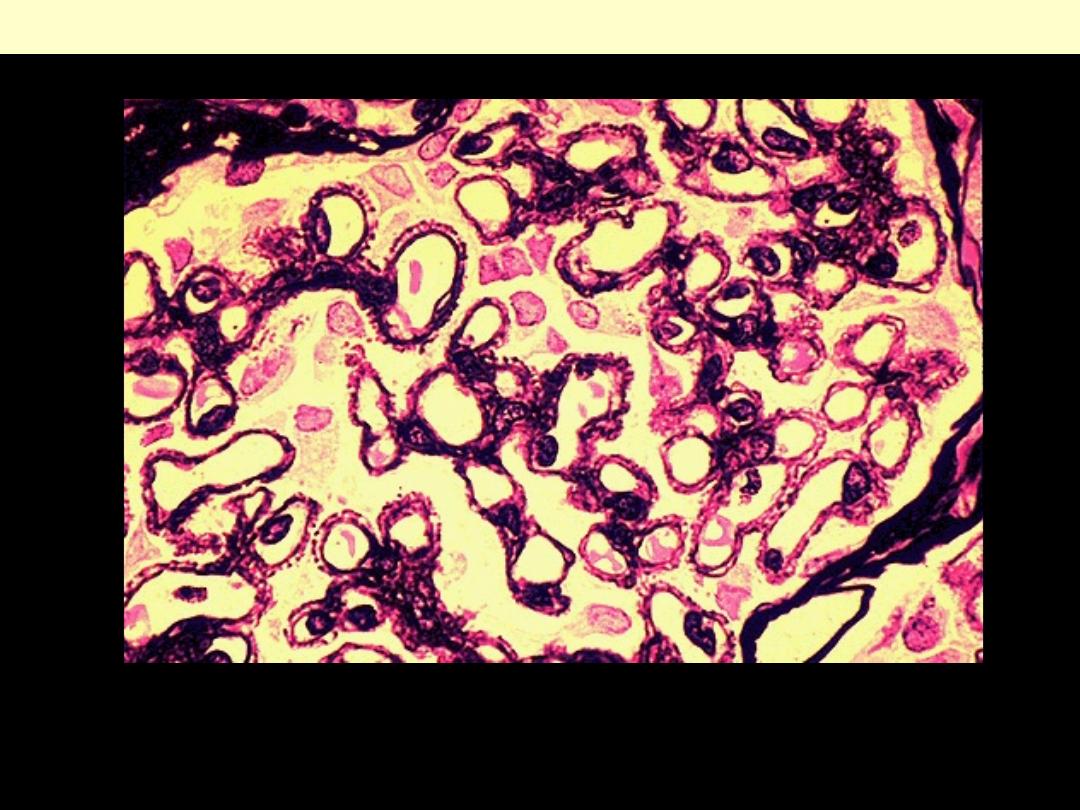
A silver stain of the glomerulus highlights the proteinaceous basement membranes in black.
There are characteristic "spikes" seen with membranous glomerulonephritis seen here in
which the black basement membrane material appears as projections around the capillary
loops.
Membranous nephropathy
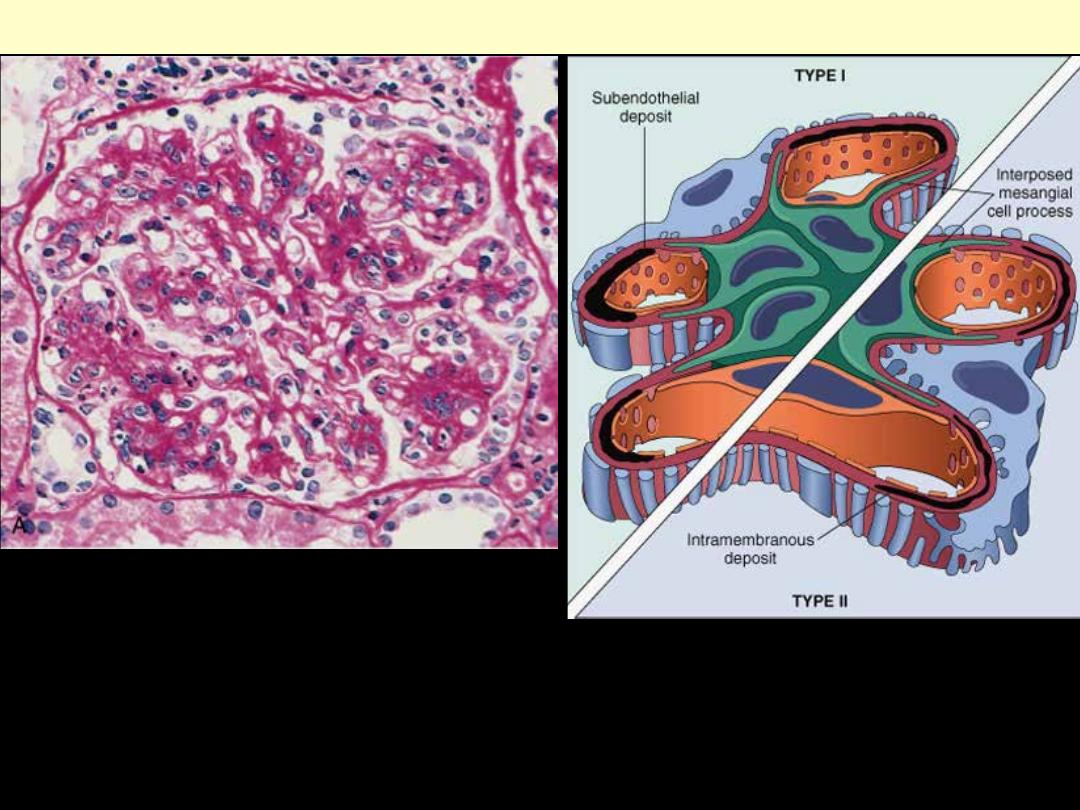
A, showing mesangial cell proliferation, basement membrane thickening, leukocyte infiltration, and
accentuation of lobular architecture. B, Schematic representation of patterns in the two types of
membranoproliferative GN. In type I there are subendothelial deposits; type II is characterized by
intramembranous dense deposits (dense-deposit disease). In both, mesangial interposition gives the
appearance of split basement membranes when viewed by light microscopy.
Membranoproliferative GN
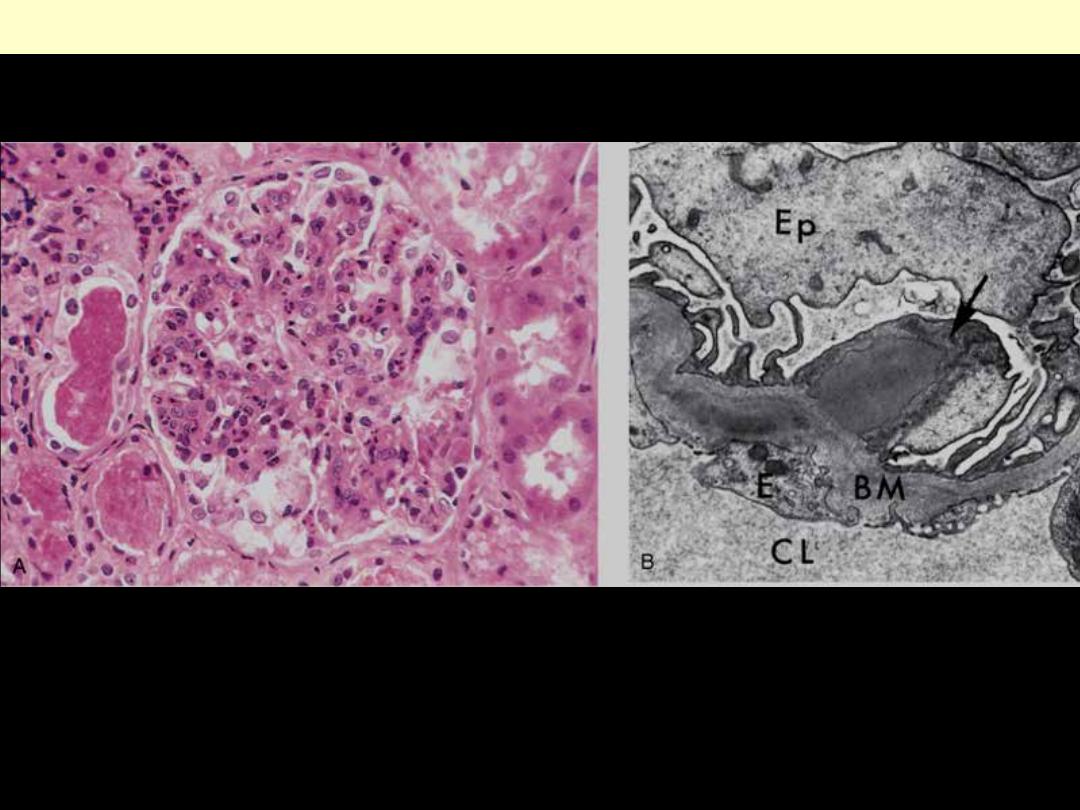
A, Glomerular hypercellularity is caused by intracapillary leukocytes and proliferation of intrinsic
glomerular cells. Note the red cell casts in the tubules. B, Typical electron-dense subepithelial "hump"
(arrow) and intramembranous deposits. BM, basement membrane; CL, capillary lumen; E, endothelial
cell; Ep, visceral epithelial cells (podocytes).
Acute diffuse post-streptococcal GN
The hypercellularity of post-streptococcal glomerulonephritis is due to increased numbers
of epithelial, endothelial, and mesangial cells as well as neutrophils in and around the
capillary loops. This disease may follow several weeks after infection with certain strains of
group A beta hemolytic streptococci. Patients typically have an elevated anti-streptolysin O
(ASO) titer.
Acute postinfectious (Poststreptococcal) GN
Post-streptococcal glomerulonephritis is immunologically mediated, and the immune deposits are
distributed in the capillary loops in a granular, bumpy pattern because of the focal nature of the
deposition process.
Acute post-infectious (Poststreptococcal) GN
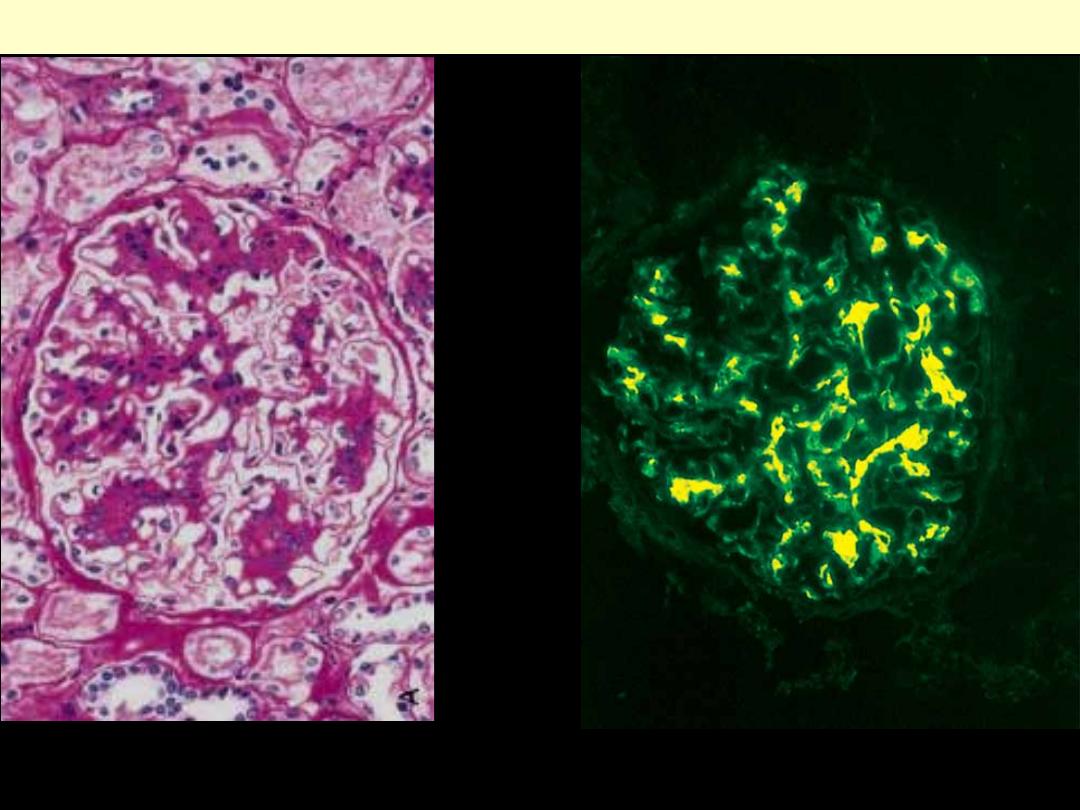
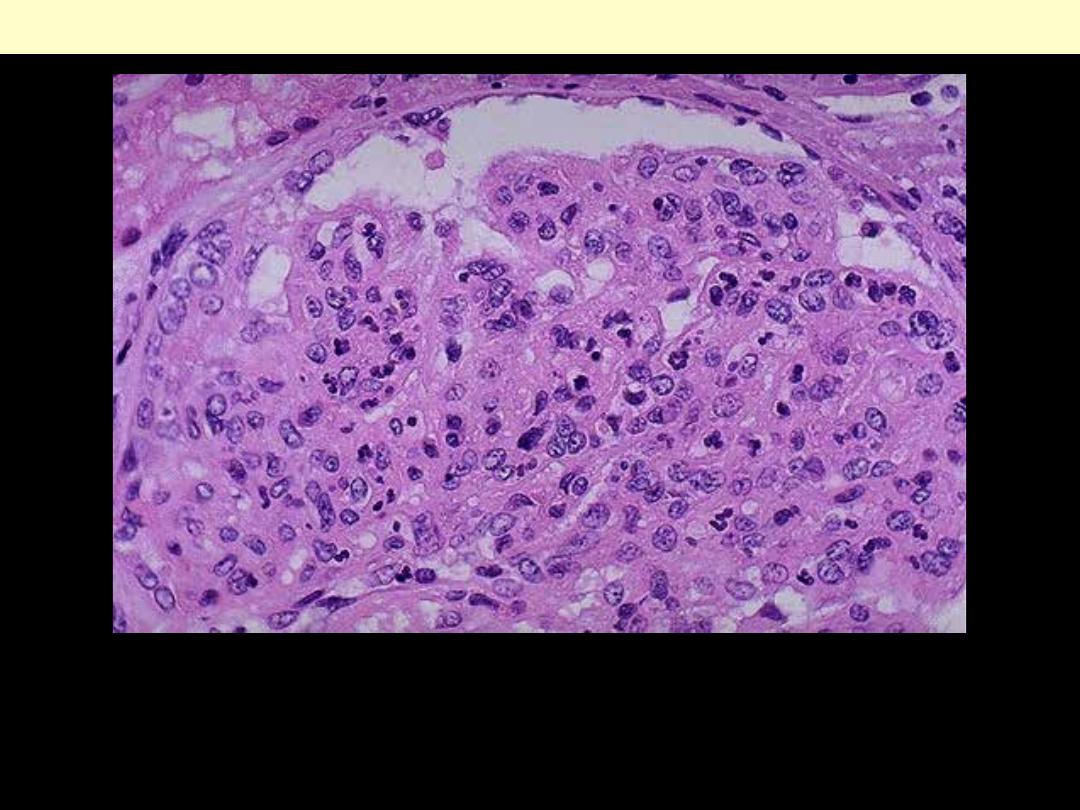
A, Light microscopy showing mesangial proliferation and matrix increase.
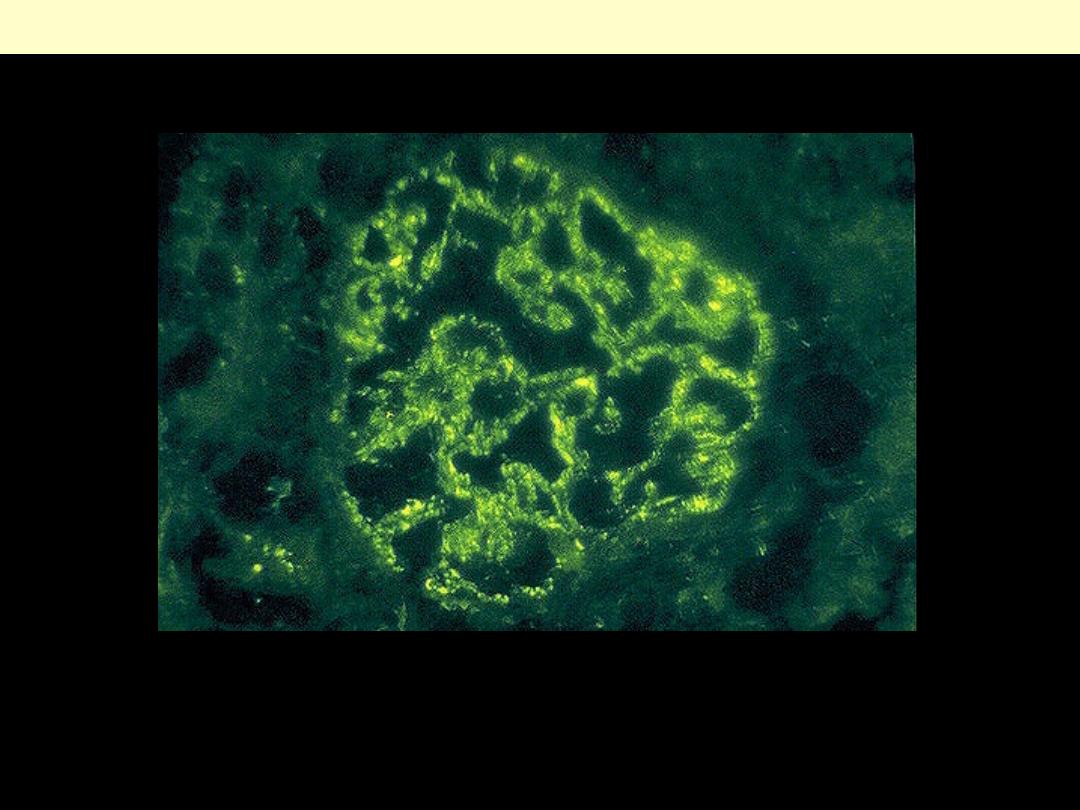
B. There is characteristic immunofluorescence deposition of IgA, principally in mesangial regions.
IgA nephropathy
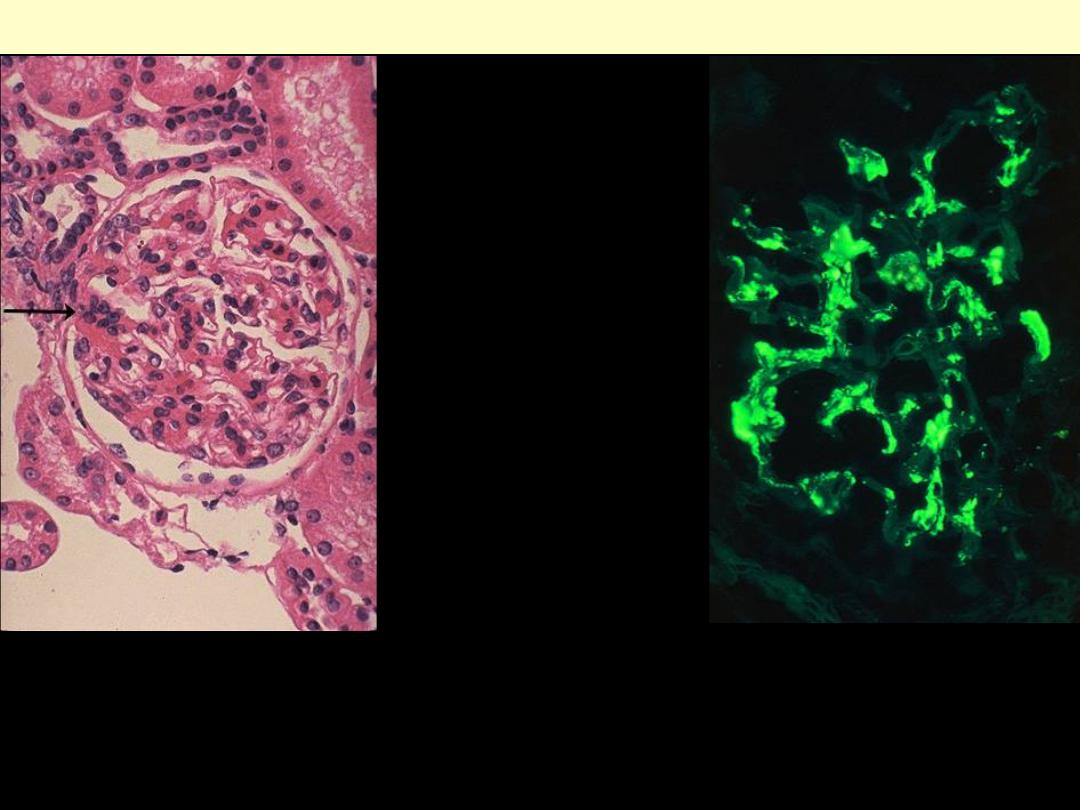
Berger's disease (IgA nephropathy)
The IgA is deposited mainly in
mesangium, which then increases
mesangial cellularity as shown at the
arrow.
This immunofluorescence micrograph
demonstrates positivity with antibody
to IgA. Note that the pattern is that of
mesangial staining.
Note the collapsed glomerular tufts and the crescent-shaped mass of proliferating cells and leukocytes
internal to Bowman's capsule.
Crescentic GN (PAS stain)
d
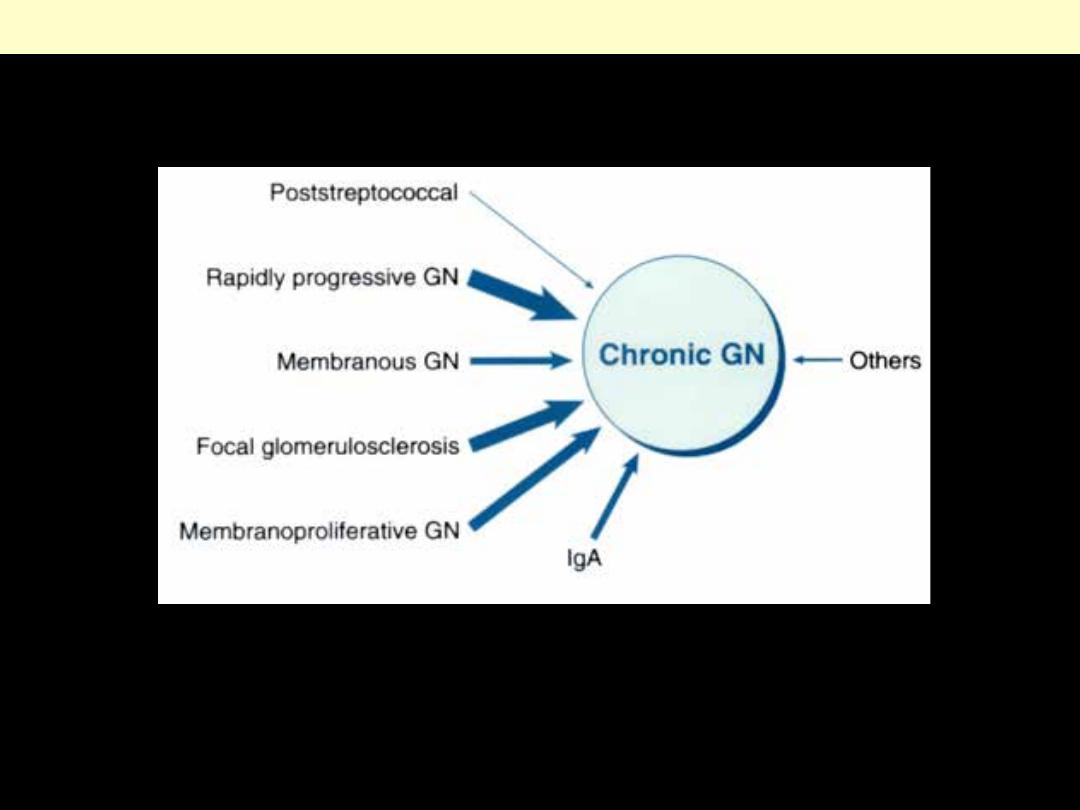
Causes of chronic GN
A Masson trichrome preparation shows complete replacement of virtually all glomeruli by blue-
staining collagen.
Chronic GN
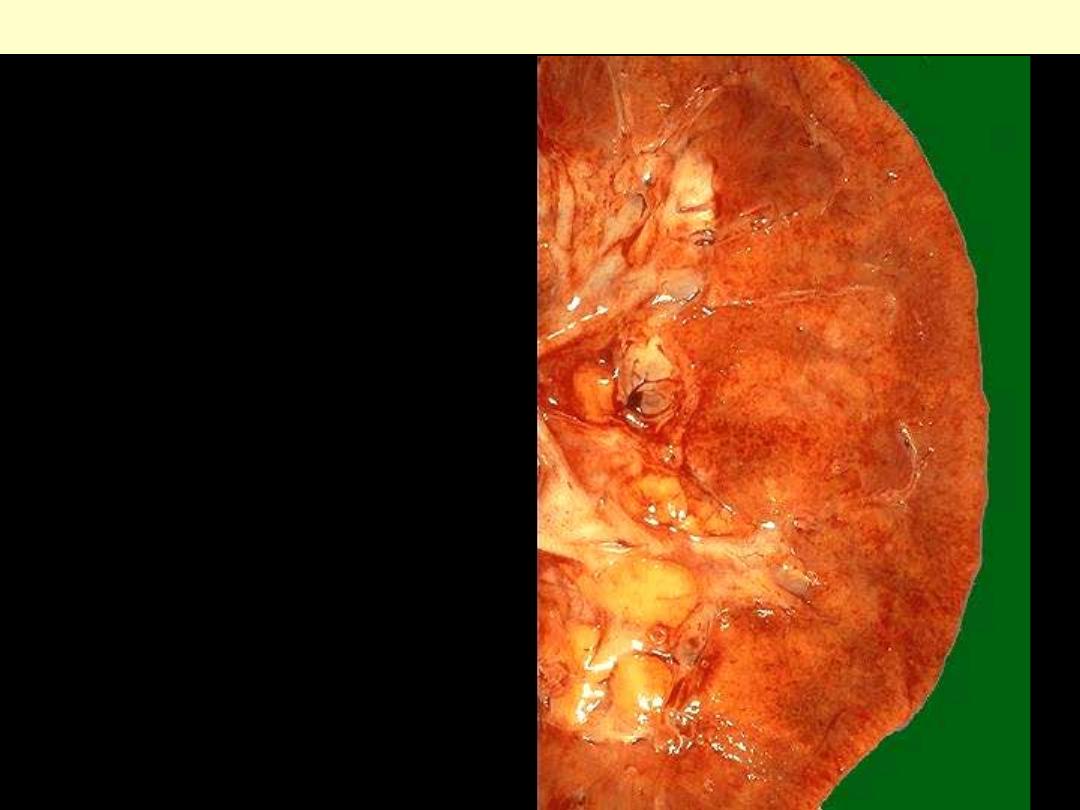
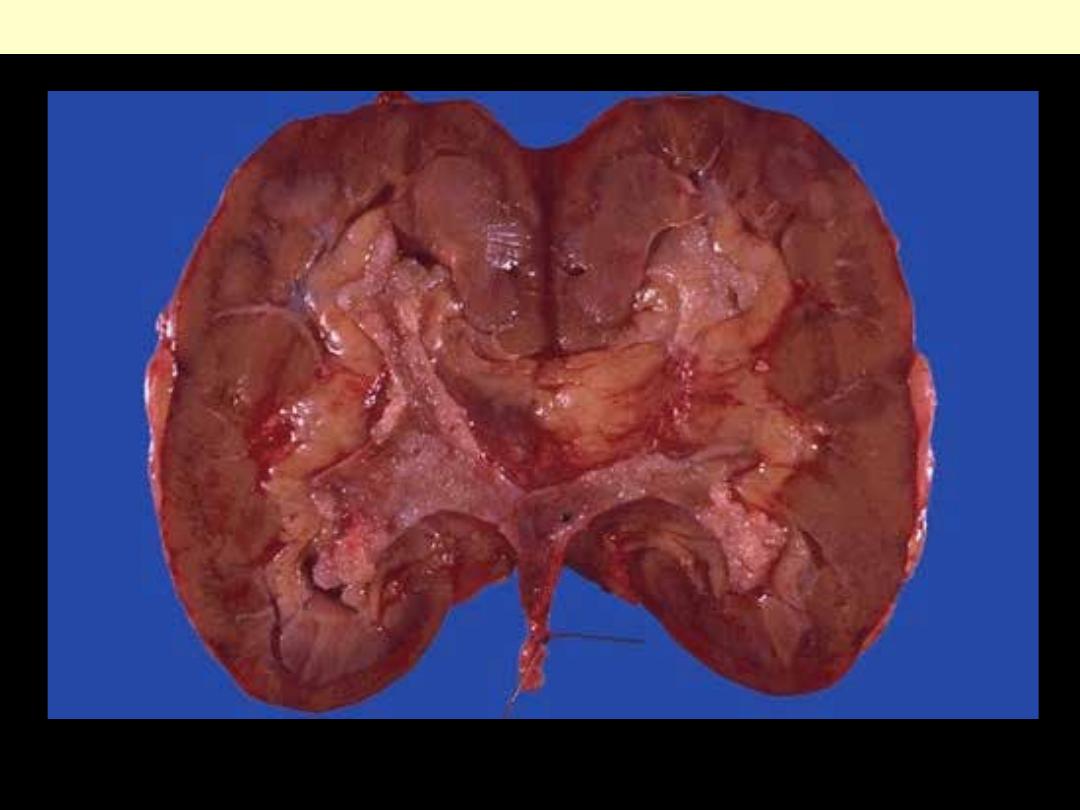
Hydronephrosis
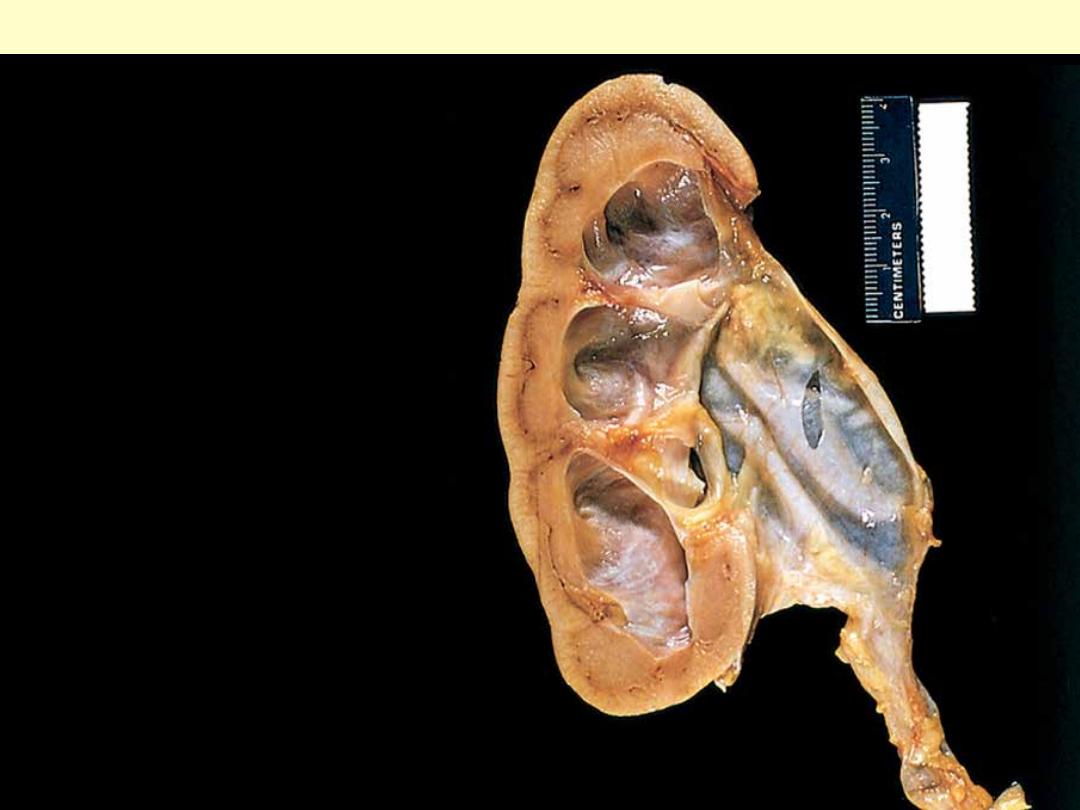
There is marked dilation of the pelvi-
calyceal system and thinning of renal
parenchyma.
Hydronephrosis of the kidney
Kidney – Cystic diseases
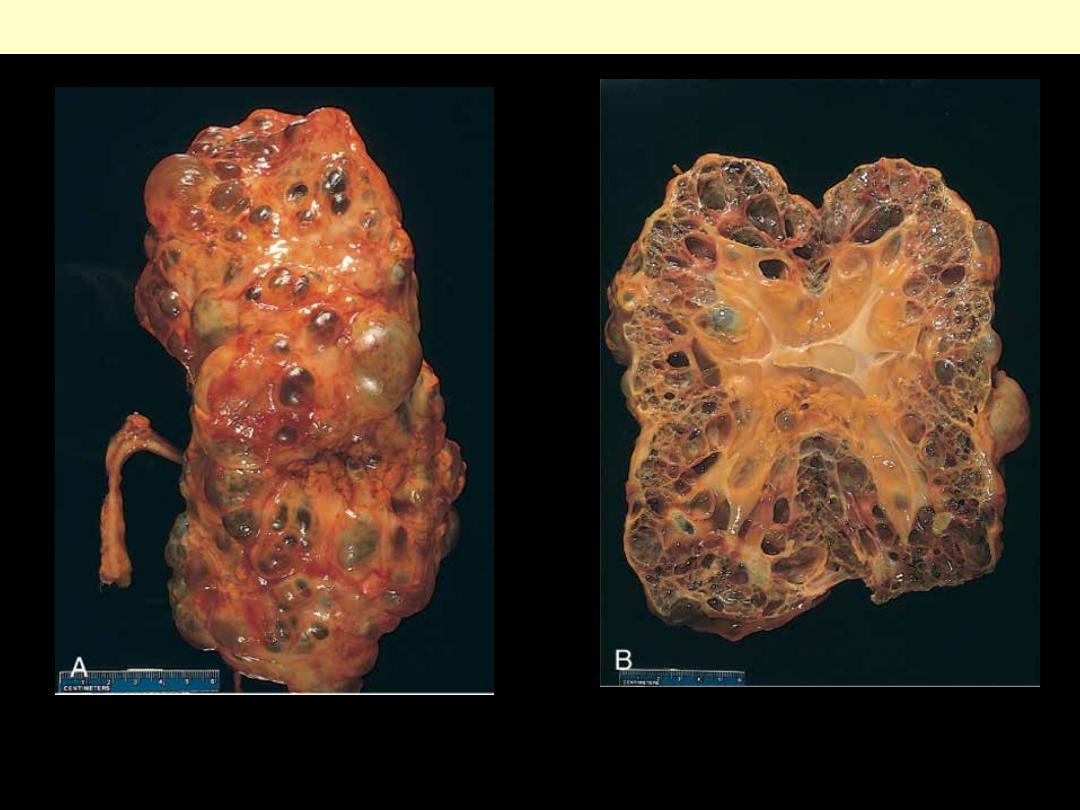
Eexternal surface (A) and bisected (B). The kidney is markedly enlarged (note the centimeter rule)
with numerous dilated cysts.
Autosomal dominant adult polycystic kidney
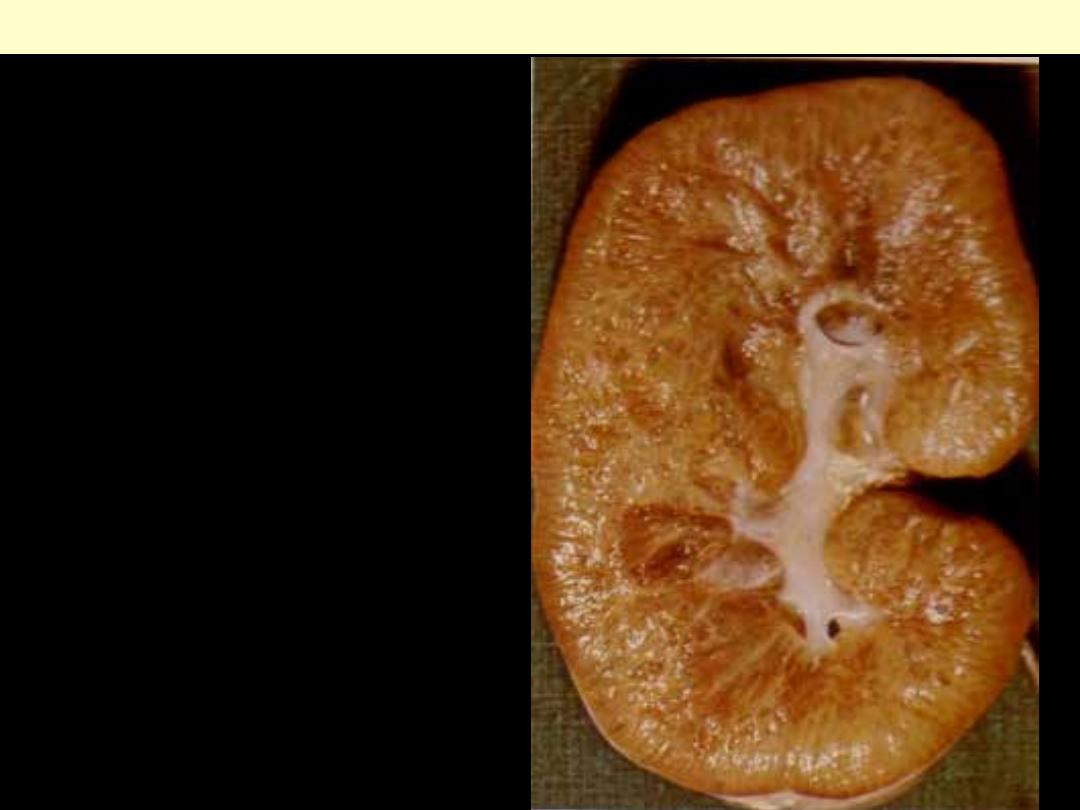
The kidney is enlarged and on section is a
sponge-like from the presence of numerous small
cysts especially in the medulla.
Autosomal Recessive Polycystic Kidney Disease (ARPKD)
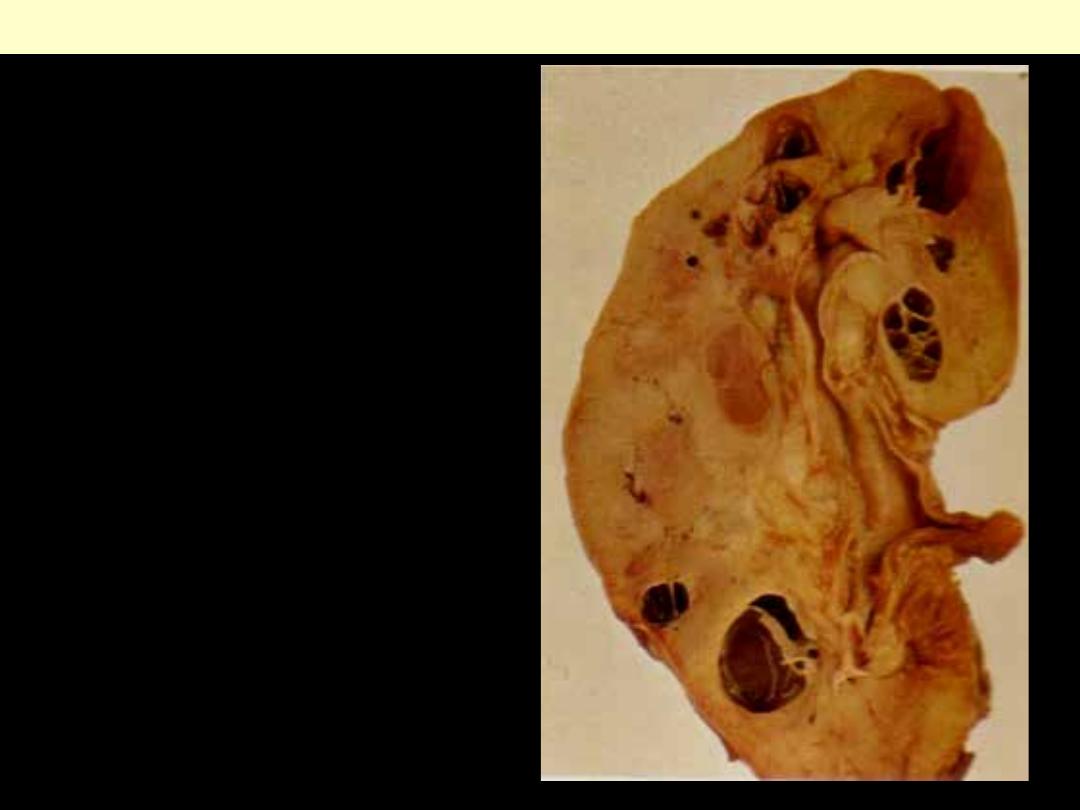
Several variably sized cysts mainly located at the
cortico-medullary junction.
Medullary cystic disease
Kidney - Tumors
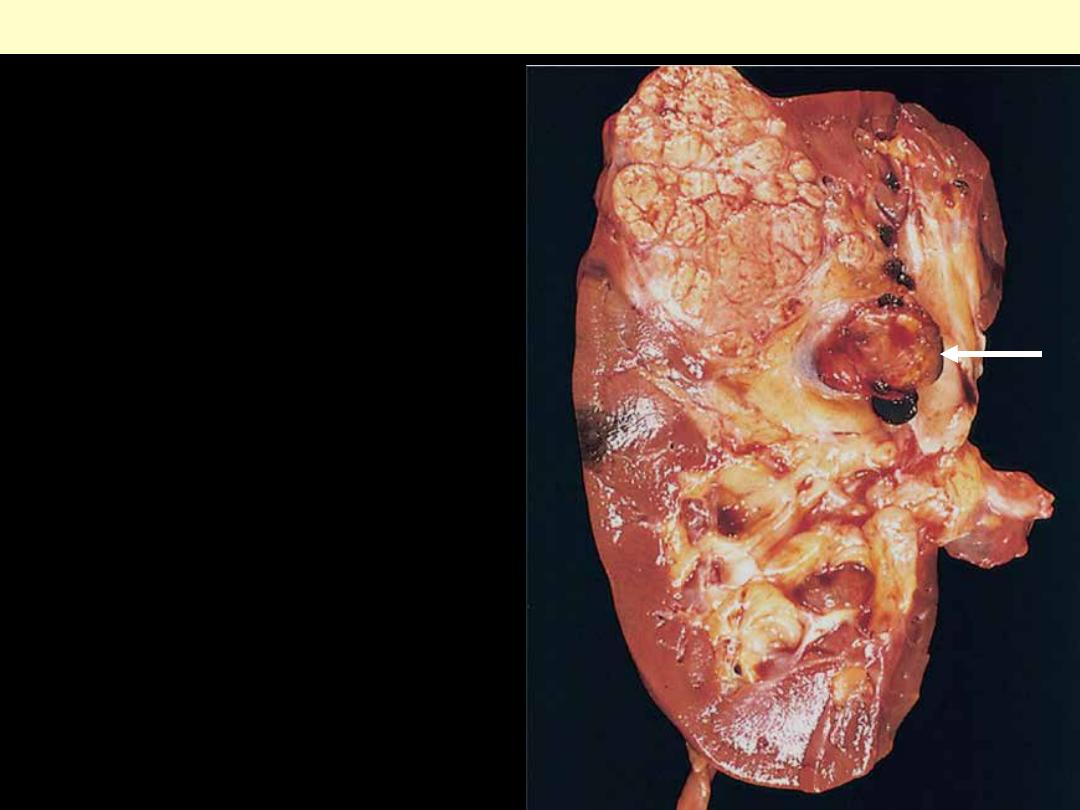
Typical cross-section of yellowish, spherical
neoplasm in one pole of the kidney. Note the
tumor in the dilated, thrombosed renal vein
(arrow).
Renal cell carcinoma
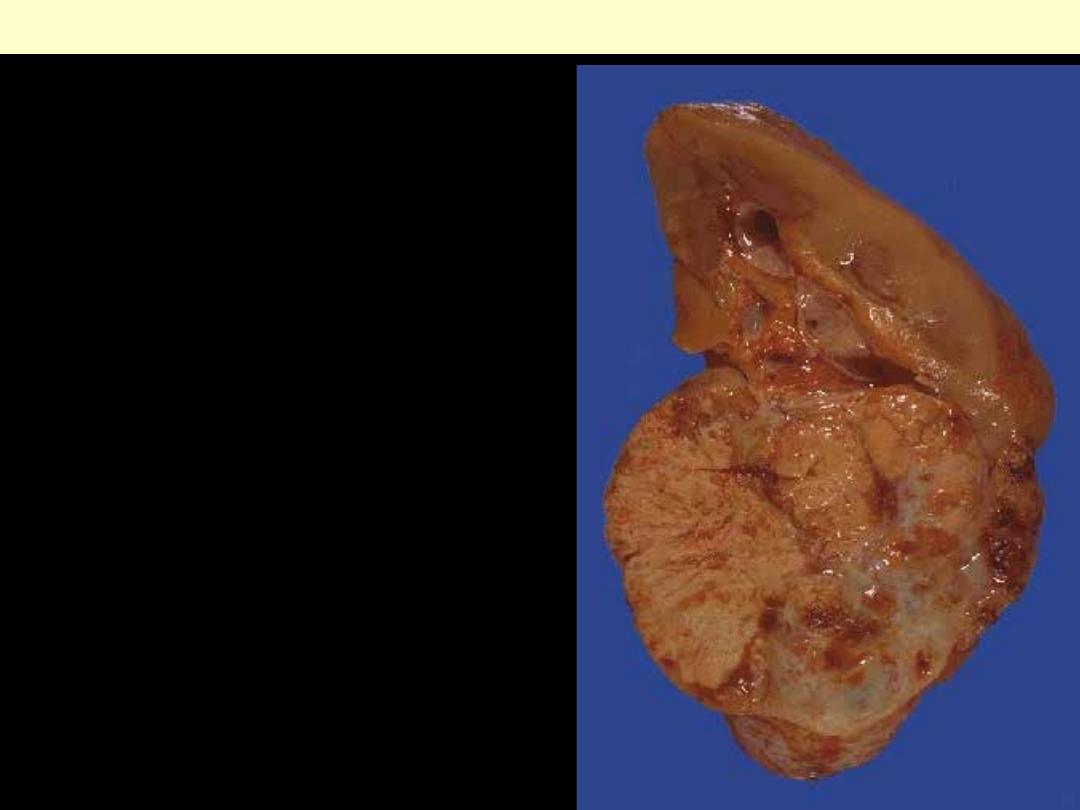
The tumor is arising in the lower pole of the kidney.
It is fairly circumscribed. The cut surface
demonstrates a variegated appearance with yellowish
areas, white areas, brown areas, and hemorrhagic red
areas. Though these neoplasms are usually slow-
growing, they can often reach a considerable size
before detection because there is a lot of room to
enlarge in the retroperitoneum and there is another
kidney to provide renal function. Thus, presenting
symptoms and signs usually include flank pain, mass
effect, and hematuria.
Renal cell carcinoma
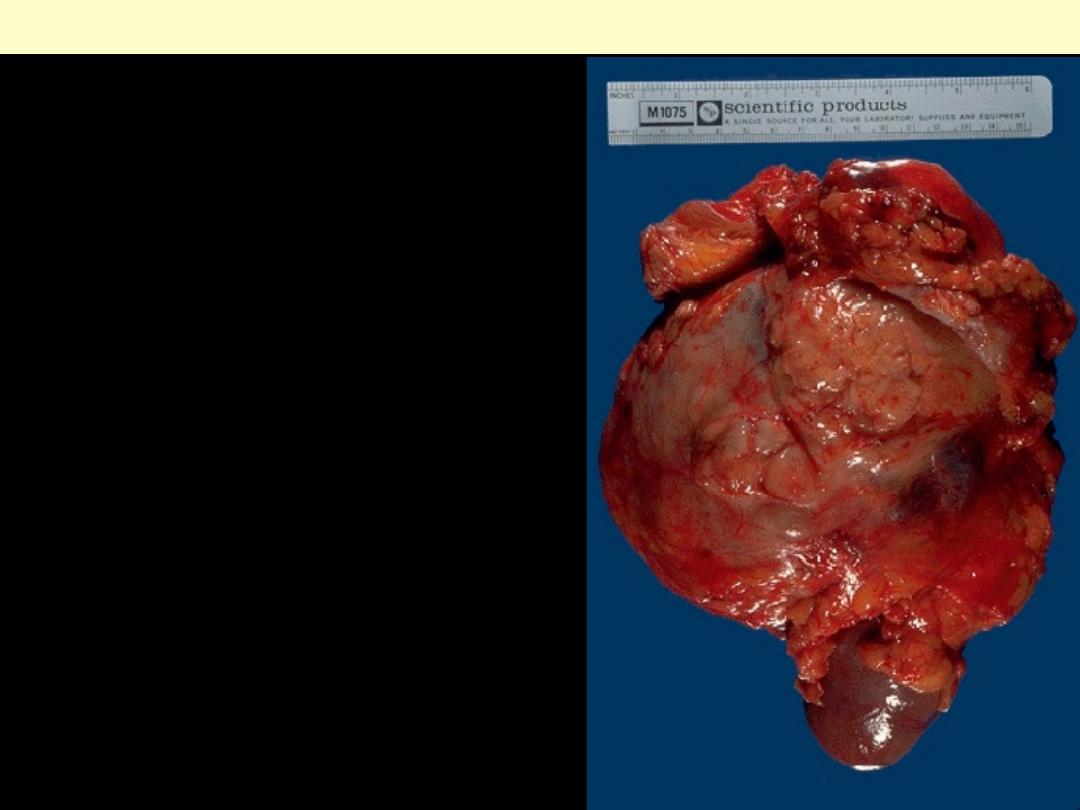
This renal cell carcinoma is very large, as indicated
by the 15 cm ruler. A portion of normal kidney
protrudes at the lower center. This patient was a
physician himself and just didn't have any early
symptoms.
Renal cell carcinoma
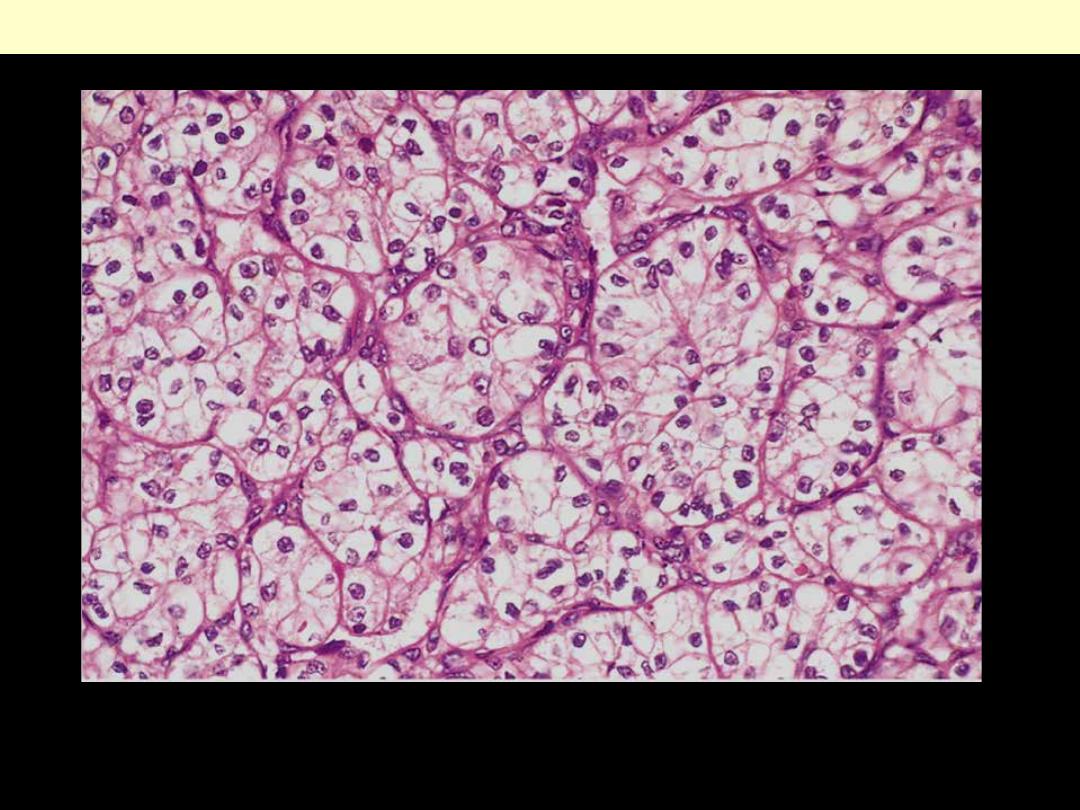
Well-defined nests of the tumor cells that appear clear (lipid-laden) with well defined cell membranes.
The nuclei are usually small and round
Renal cell carcinoma, clear cell type
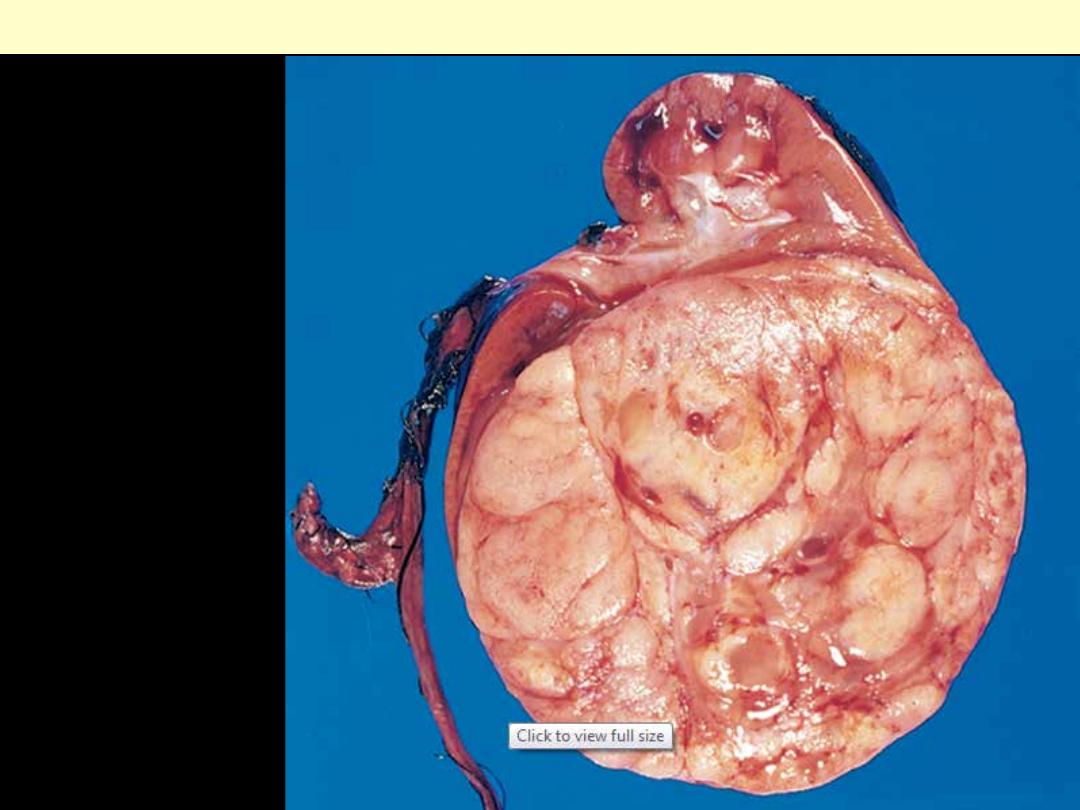
The tumor is in the
lower pole of the kidney
with the characteristic
tan to gray color and
well-circumscribed
margins.
Wilms' tumor
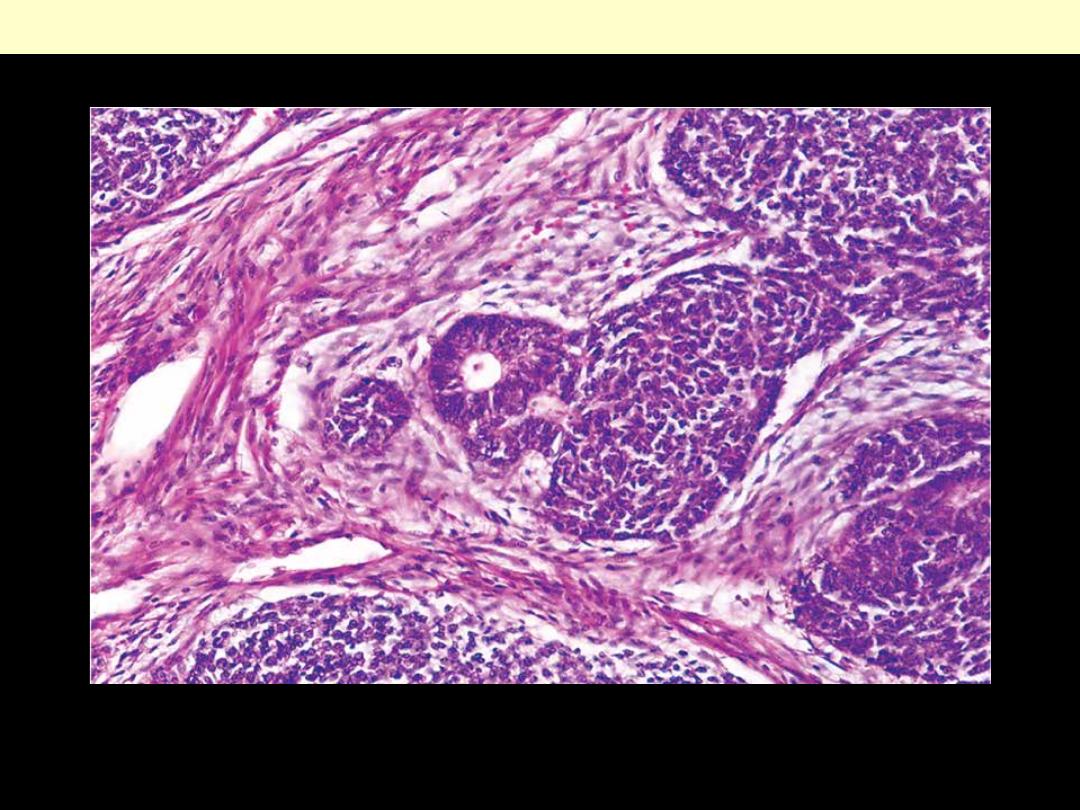
Triphasic histology of Wilms' tumor: the stromal component is composed of spindle-shaped cells in the
less cellular area on the left; the immature tubule in the center is an example of the epithelial
component, and the tightly packed blue cells the blastemal elements.
Wilms' tumor
Nephrosclerosis
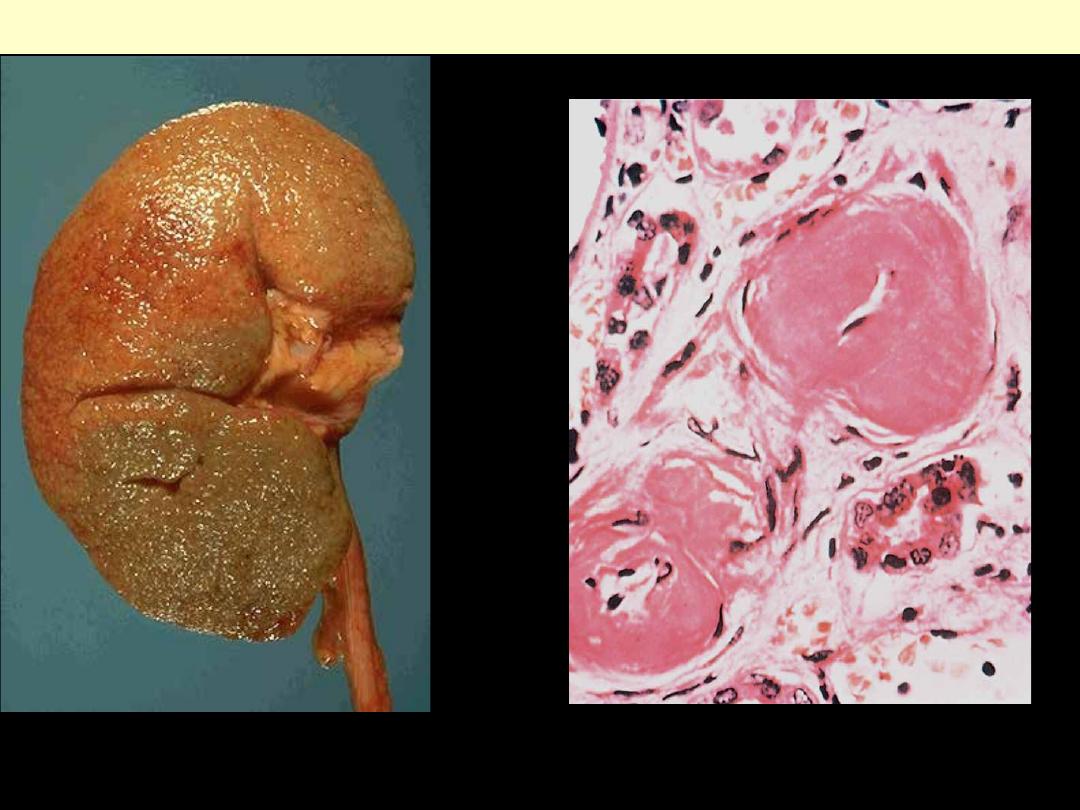
The cortical surface in benign nephrosclerosis
illustrating the fine, leathery granularity of the
surface.
Benign nephrosclerosis
High-power view of two arterioles with
hyaline deposition, marked thickening of the
walls, and a narrowed lumen.
Section of the kidney demonstrating focal small
hemorrhages (flea bitten kidney).
Malignant nephrosclerosis
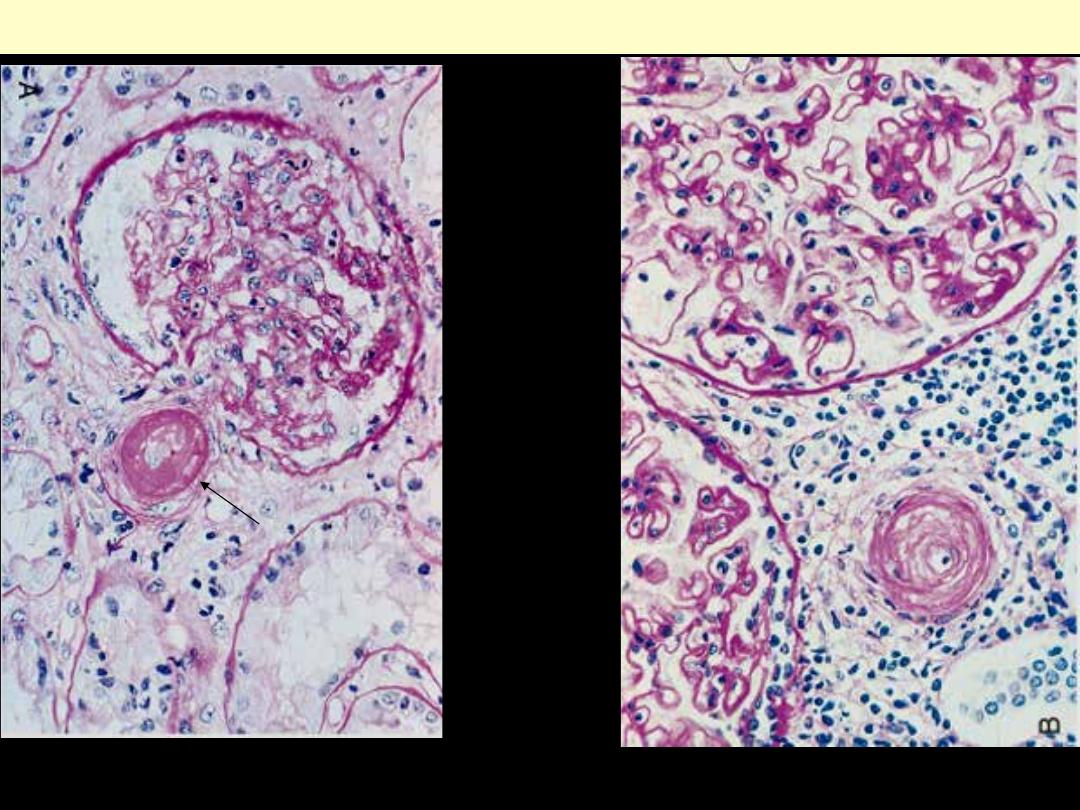
A, Fibrinoid necrosis of afferent arteriole (PAS stain). B, Hyperplastic arteriolosclerosis (onion-skin
lesion)
Malignant nephrosclerosis
Malignant nephrosclerosis
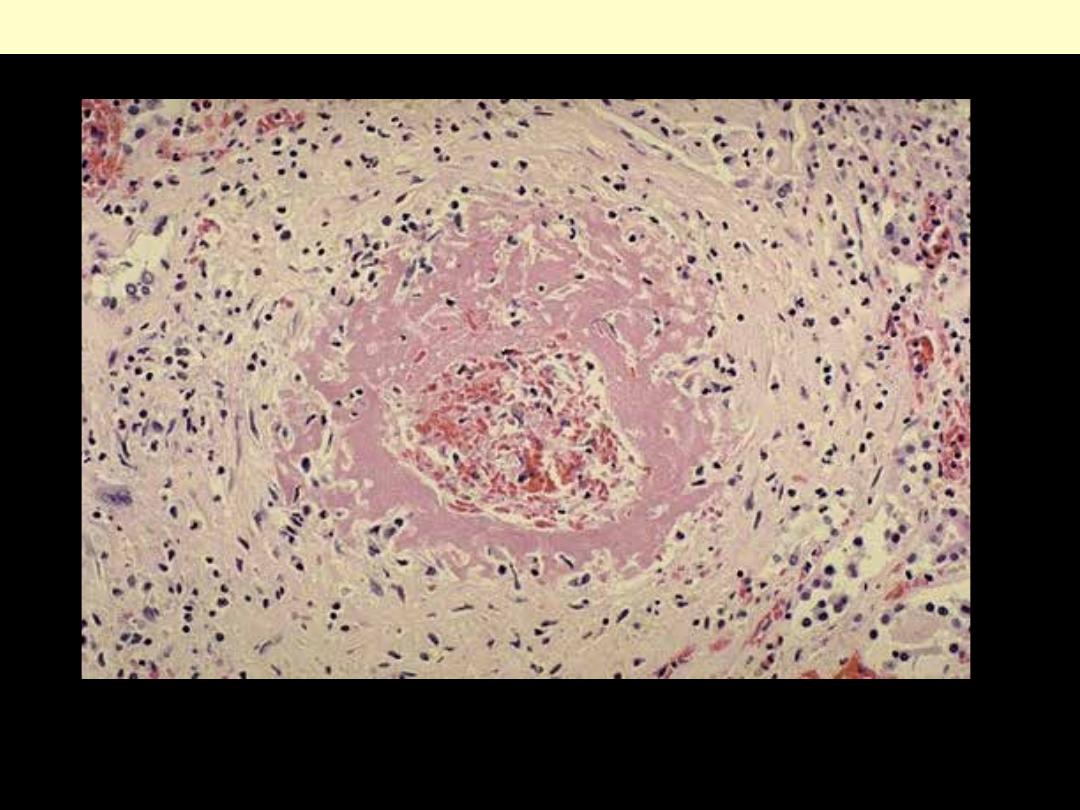
malignant hypertension with fibrinoid necrosis of a renal arteriole.
Malignant nephrosclerosis
Renal stones
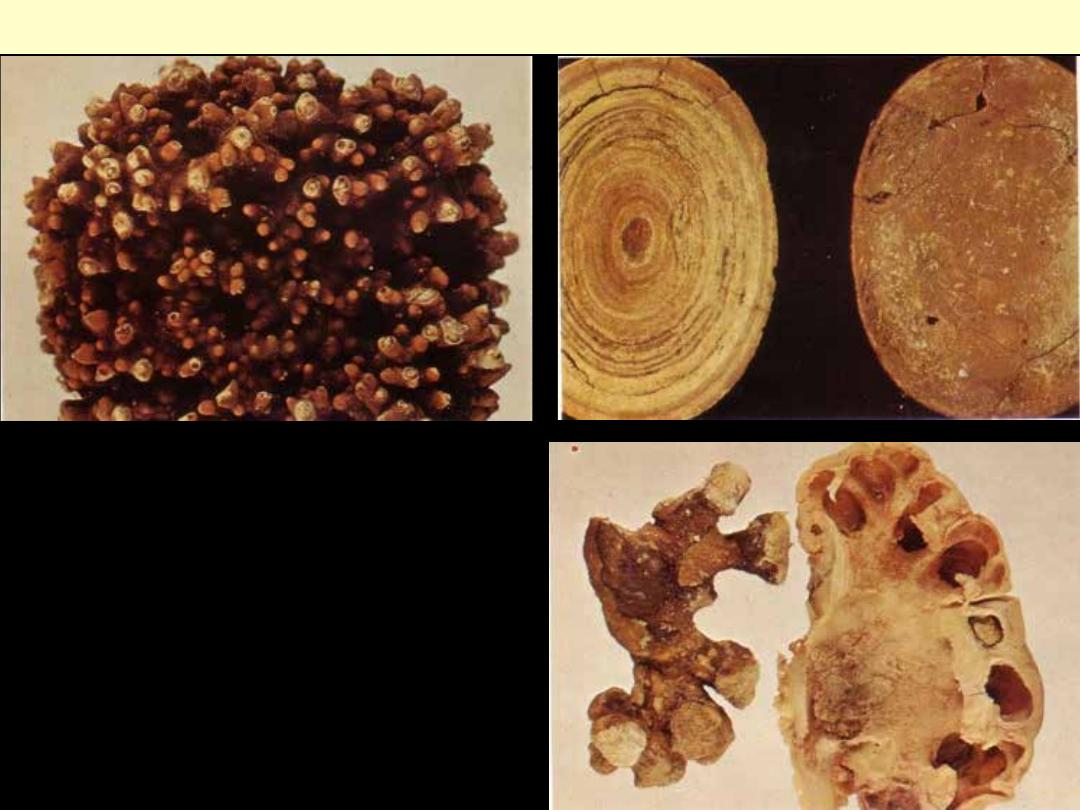
Upper left: Oxalate stone
Upper Rt. Uric acid stone
Lower Rt. A staghorn phosphate stone
Renal stones
Tubulointerstitial nephritis
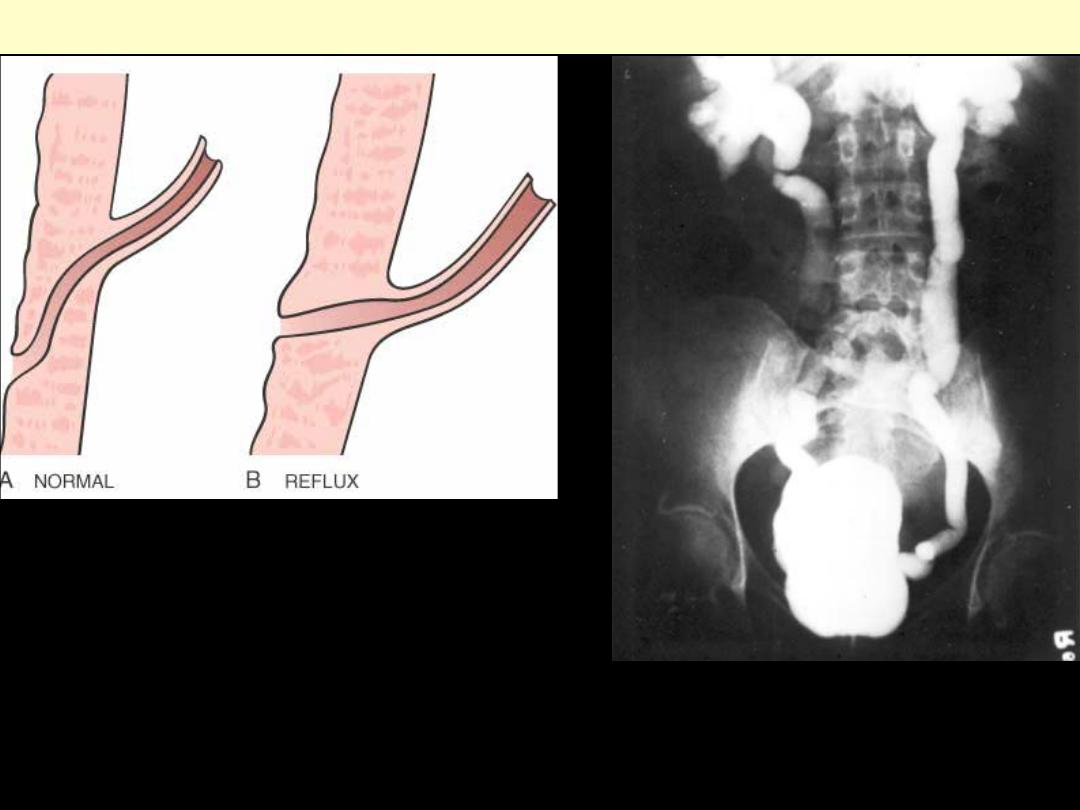
The vesicoureteral junction. In normal individuals
(A), the intravesical portion of the ureter is oblique,
such that the ureter is closed by muscle contraction
during micturition. The most common cause of
reflux is congenital complete or partial absence of
the intravesical ureter (B).
Vesicoureteral reflux
Vesicoureteral reflux demonstrated by a
voiding cystourethrogram. Dye injected
into the bladder refluxes into both dilated
ureters, filling the pelvis and calyces.

Rt. The cortical surface is studded with focal pale abscesses, more numerous in the upper pole and
middle region of the kidney; the lower pole is relatively unaffected. Between the abscesses there is dark
congestion of the renal surface.
Lt. Cut section showing multiple small yellow abscess mainly in the cortex but also in the medulla. Note
the markedly congested parenchyma & pelvic mucosa.
Acute pyelonephritis
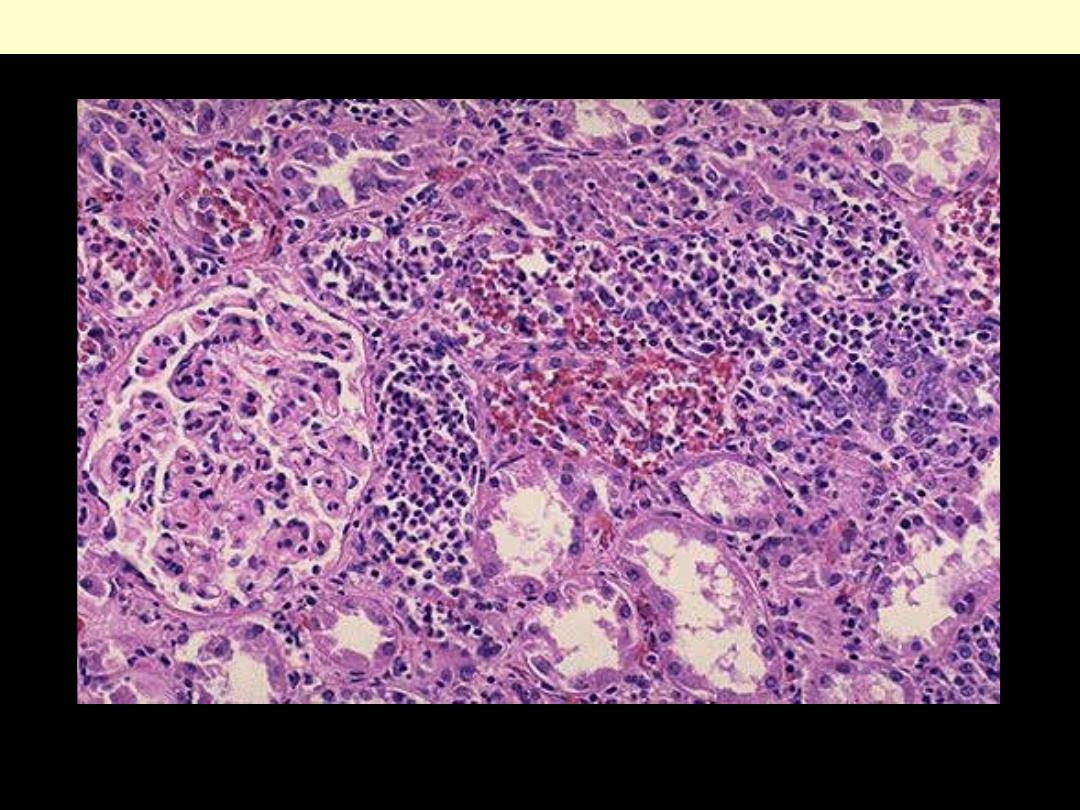
There is intense acute neutrophilic infiltration within tubules and the renal substance.
Acute Pyelonephritis
Areas of pale gray necrosis are limited to the
papillae. The distal part of each pyramid is
greyish white and necrotic.
Papillary necrosis
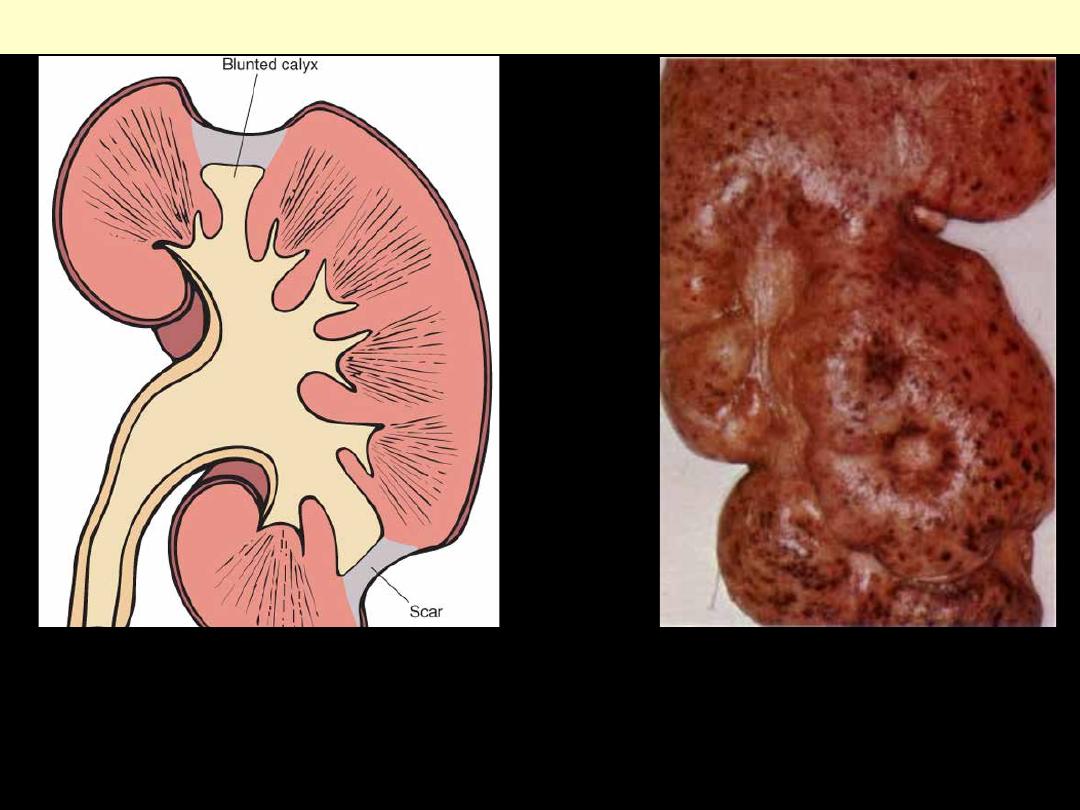
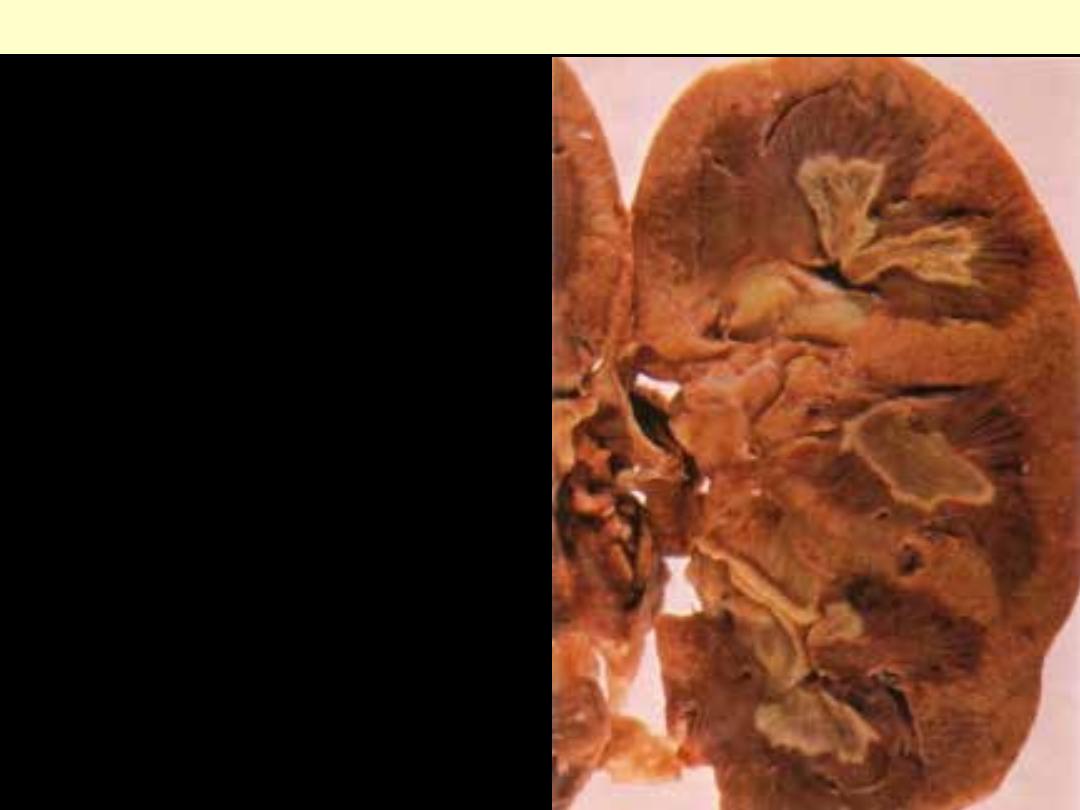
Typical coarse scars of chronic pyelonephritis
associated with vesicoureteral reflux. The scars
are usually located at the upper or lower poles of
the kidney and are associated with underlying
blunted calyces.
Chronic pyelonephritis
The cortical surface shows coarse depressed
scars, each with greyish-white center.
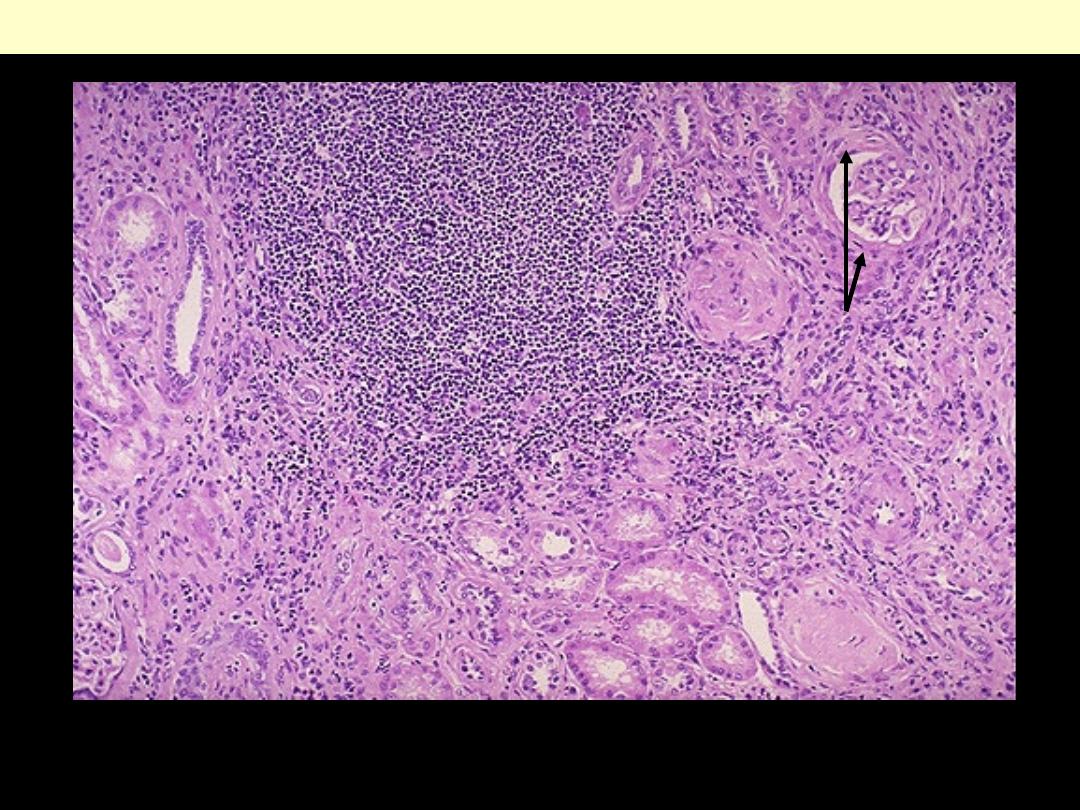
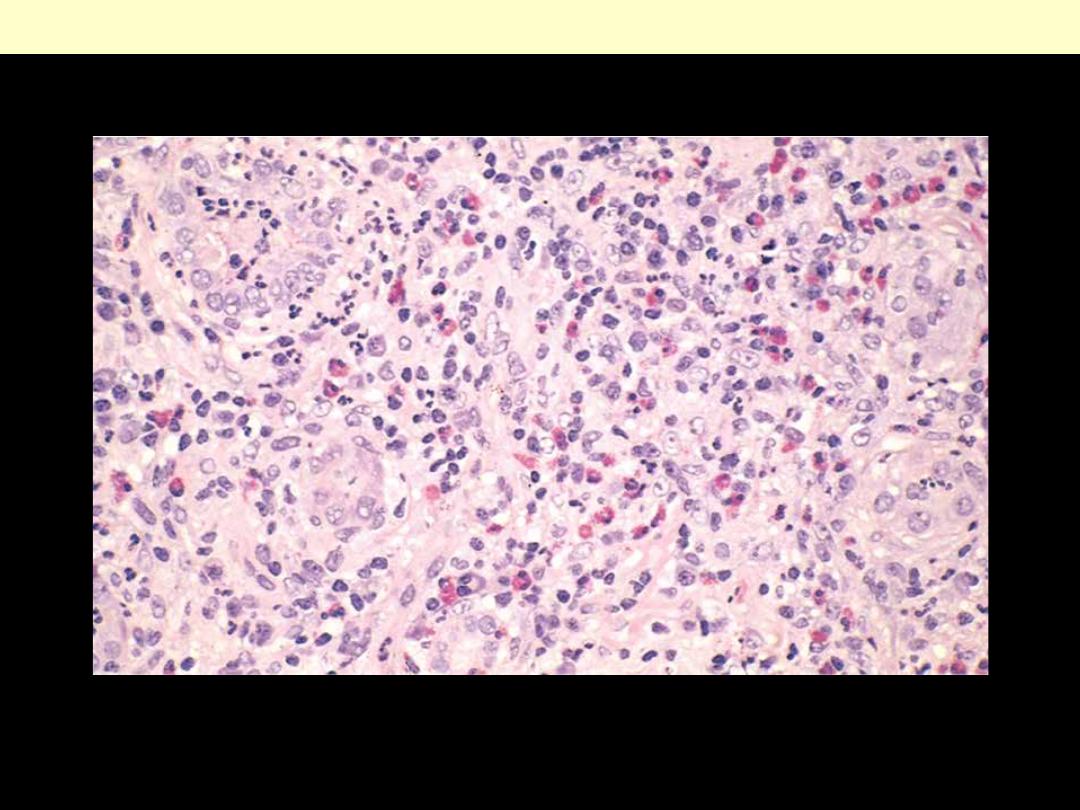
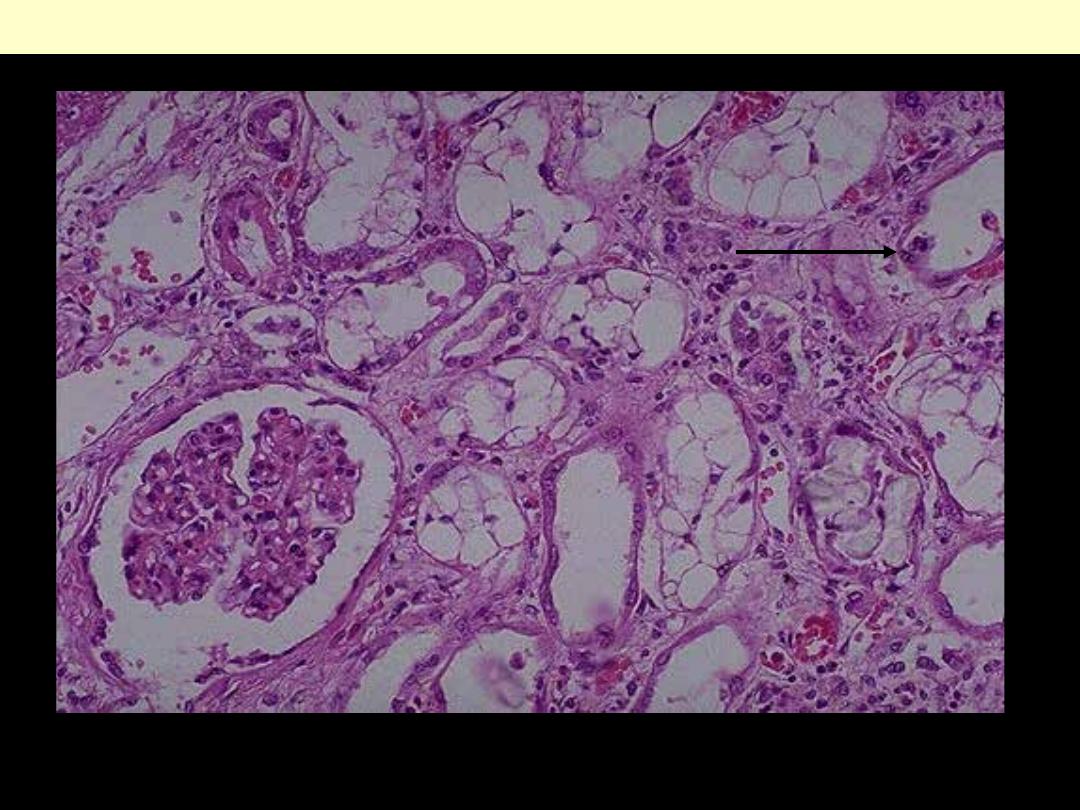
There is a large collection of chronic inflammatory cells associated with fibrosis that involves the
interstitum & periglomerular areas (arrow). This biopsy is from here a patient with a history of
multiple recurrent urinary tract infections.
Chronic pyelonephritis
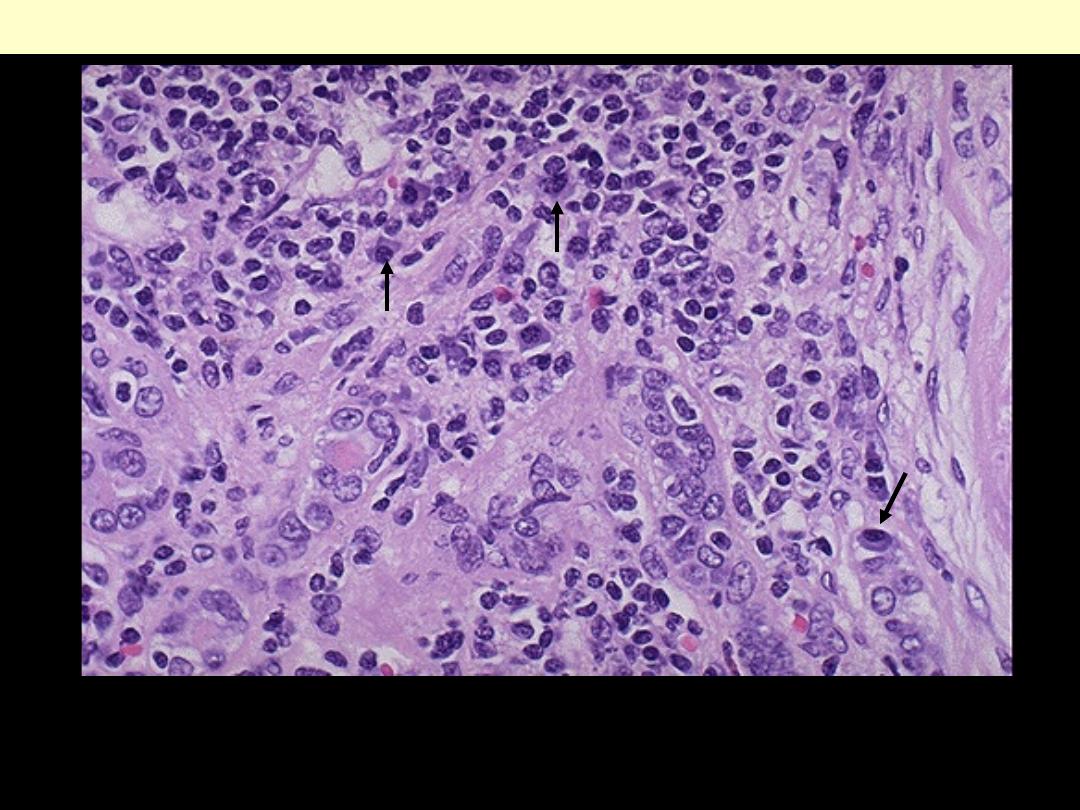
Both lymphocytes and plasma cells are seen at high magnification in this case of chronic
pyelonephritis. It is not uncommon to see lymphocytes accompany just about any chronic renal
disease: glomerulonephritis, nephrosclerosis, pyelonephritis. However, the plasma cells (arrows) are
most characteristic for chronic pyelonephritis.
Chronic pyelonephritis
There is prominent eosinophilic and mononuclear infiltrate of the interstitium
Acute drug-induced tubulo-interstitial nephritis
There is prominent vacuolization of tubular epithelial cells. Some tubules show epithelial sloughing &
regeneration (arrow).
Toxic Acute tubular necrosis due to ethylene glycol poisoning
Urinary bladder - Cystitis
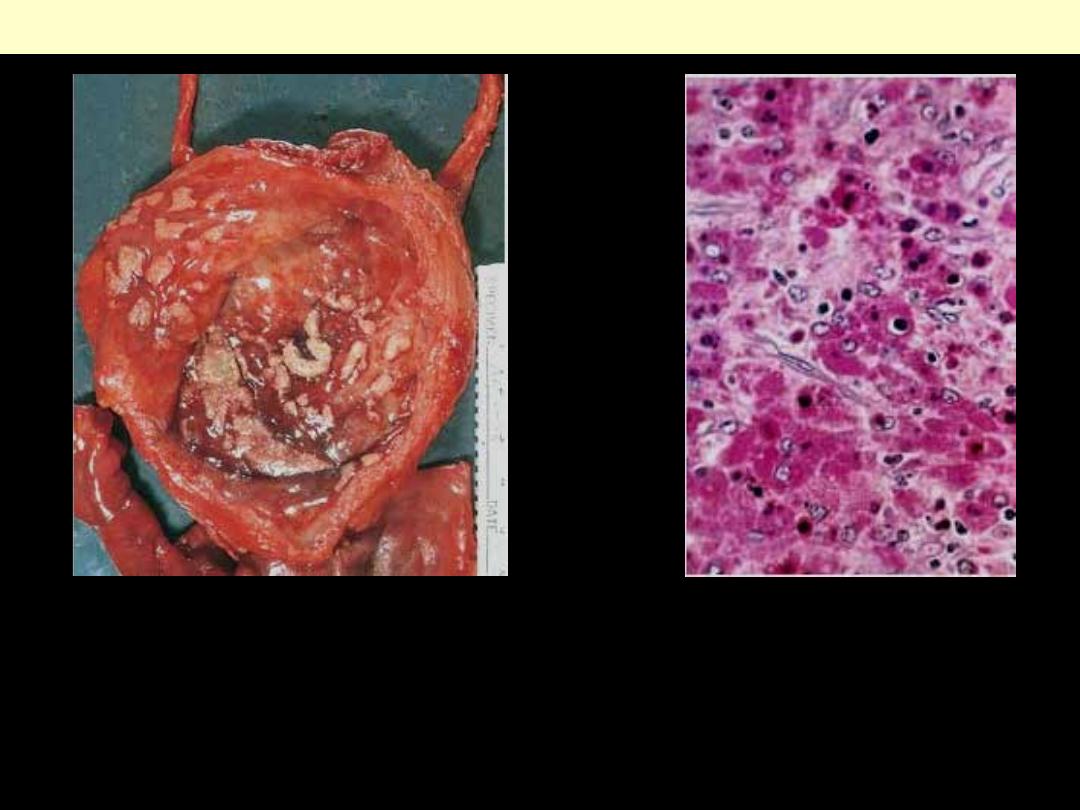
Bilharzial (“sand grain”) cystitis
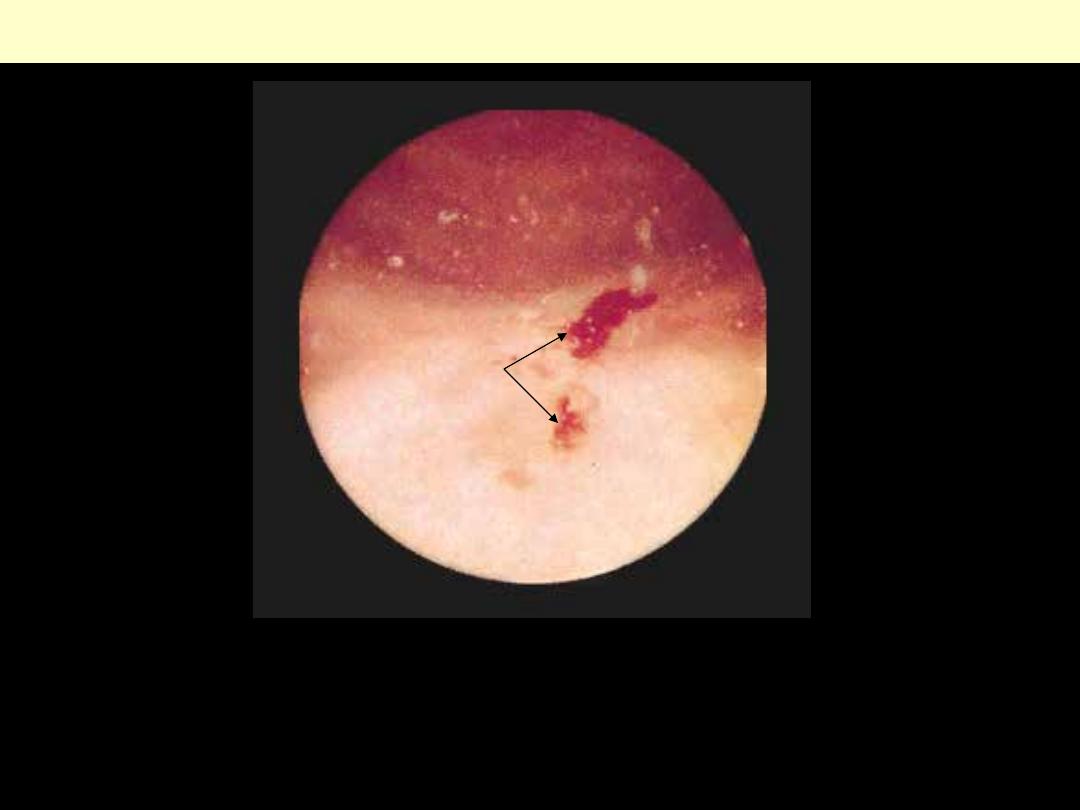
Chronic deep ulcerations of the bladder, seen through a cystoscope in a patient with S. hematobium
infection. Note the bilharzial tubercles at the top of the picture.
ulcers
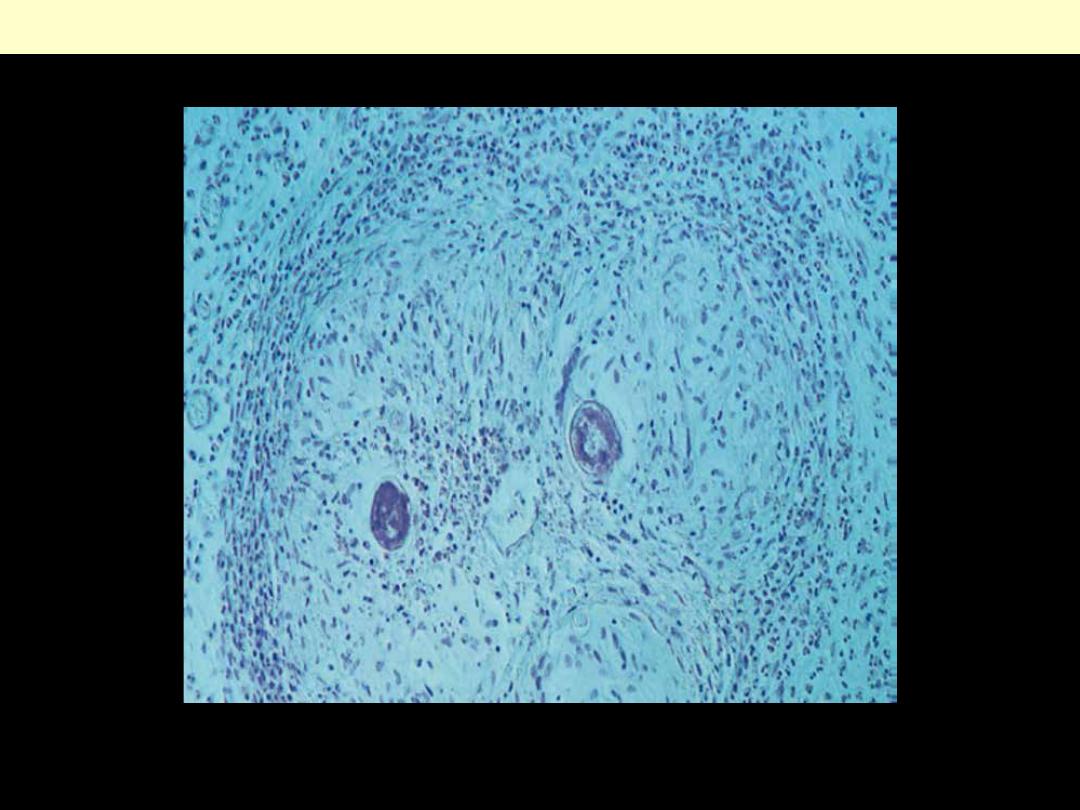
Schistosomic granuloma
(HE) x 150
d
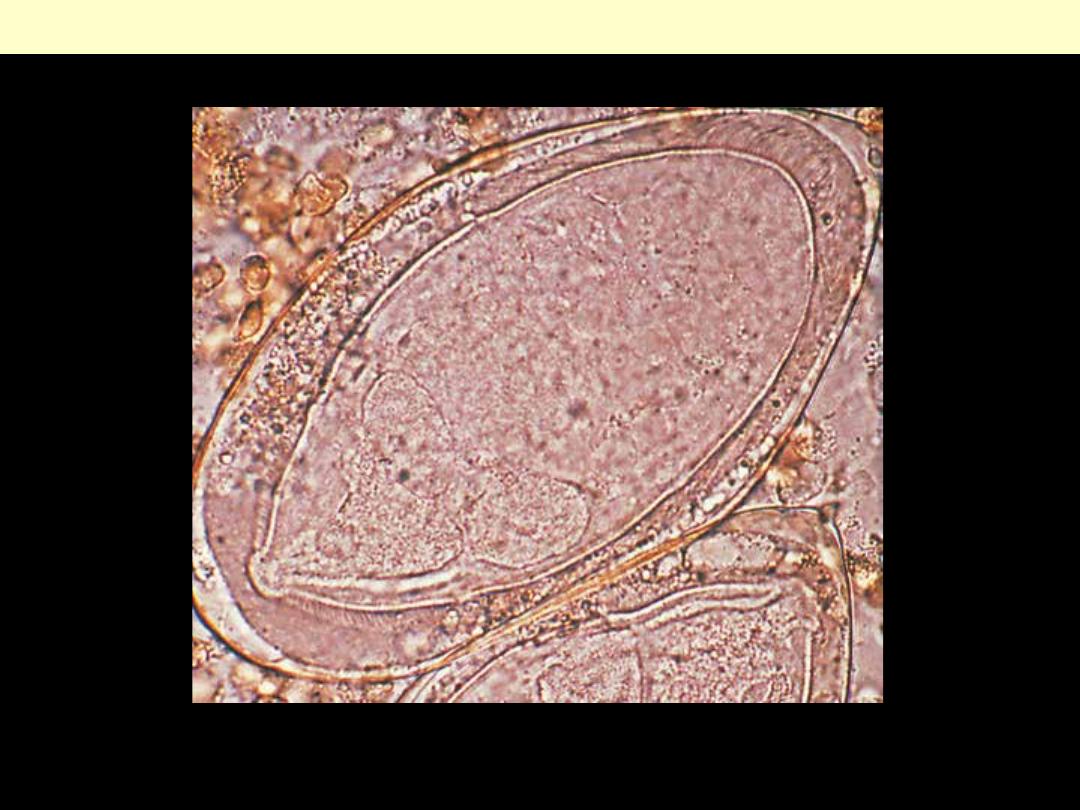
Schistosoma haematobium egg
PAS stain. Note the large macrophages
with granular PAS-positive cytoplasm
and several dense, round Michaelis-
Gutmann bodies surrounded by
artifactual cleared holes in the upper
middle field.
Malacoplakia
Cystitis with malacoplakia of bladder
showing inflammatory exudate and
broad, flat plaques.
Urinary bladder – Tumors
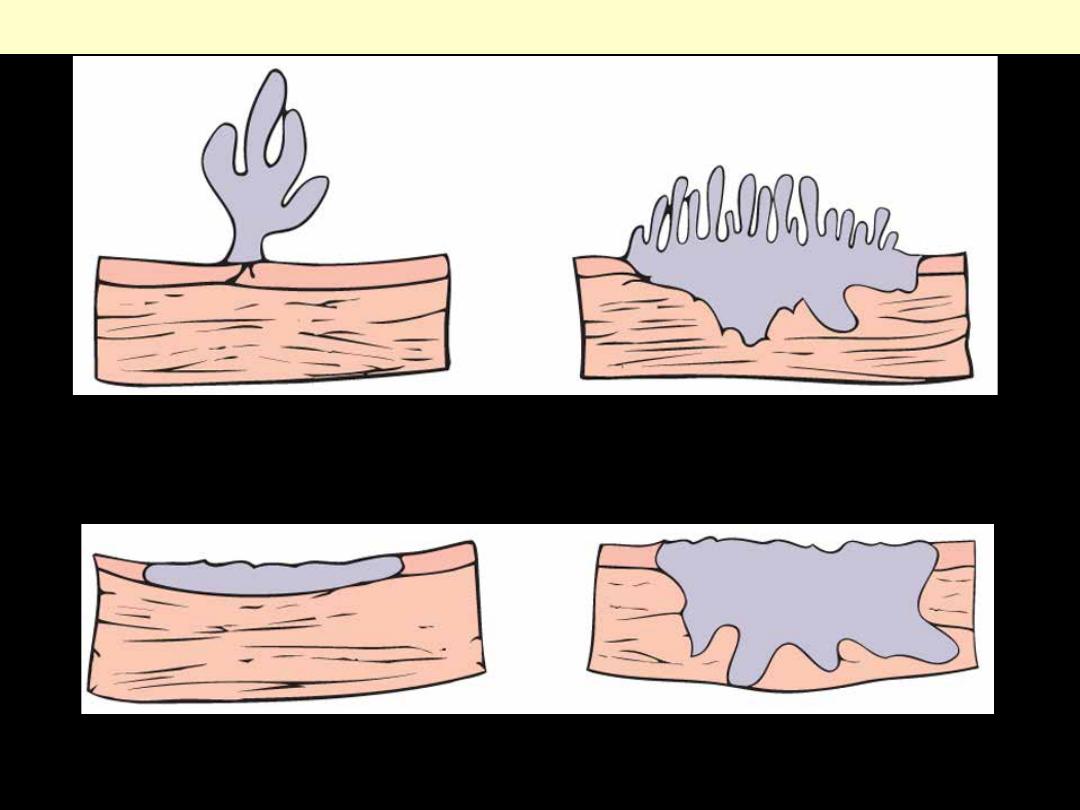
Flat non-invasive carcinoma
Flat invasive carcinoma
Morphologic patterns of bladder tumor
Papilloma-papillary carcinoma
Invasive papillary carcinoma
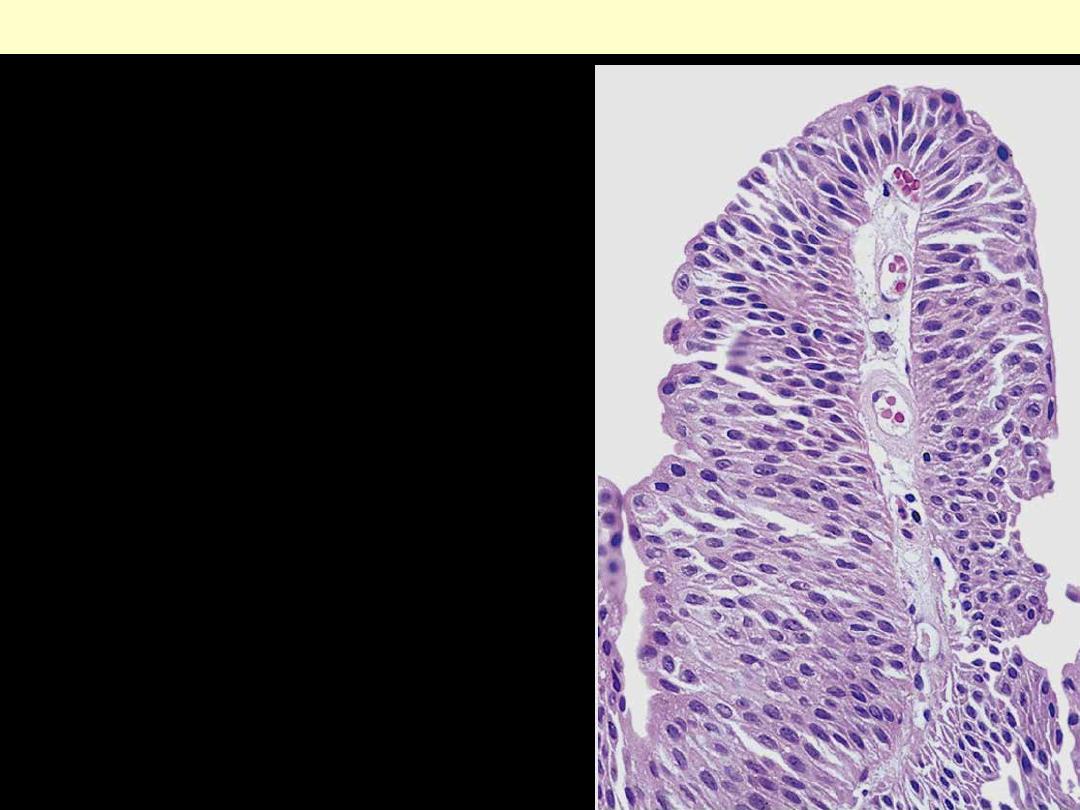
The delicate papilla is covered by orderly transitional
epithelium.
Low-grade papillary urothelial carcinoma of the bladder
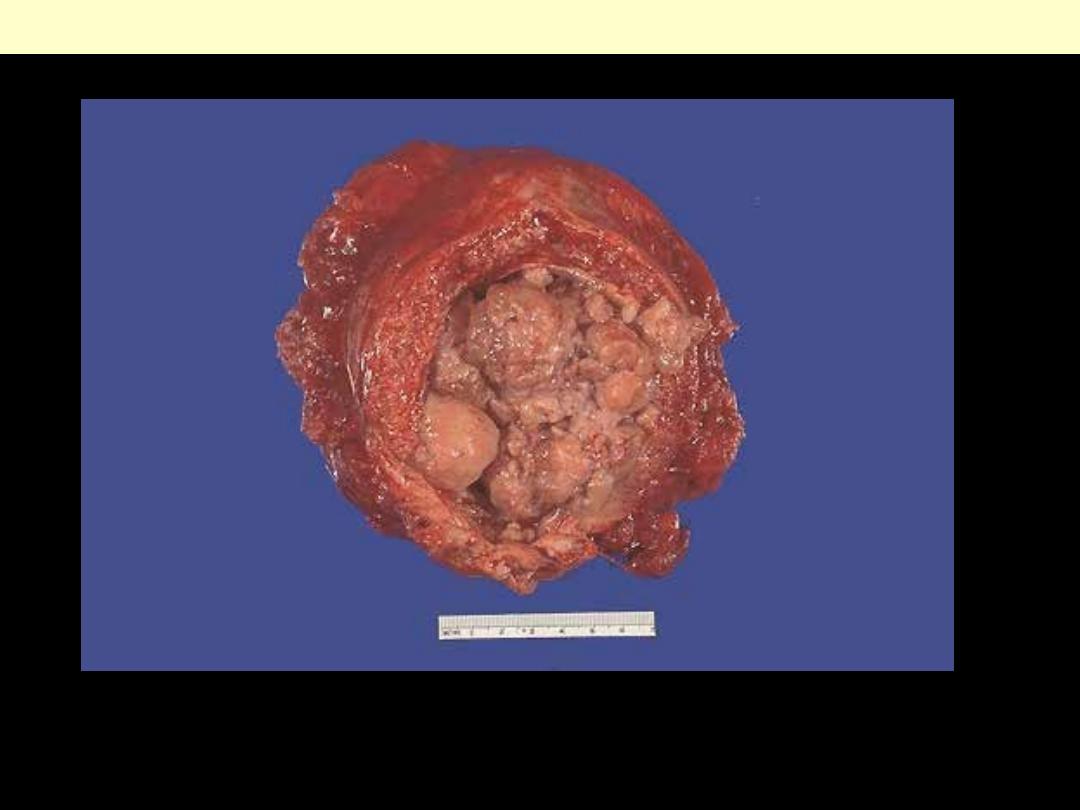
This bladder was removed surgically from a male who had a long history of smoking. He had presented
with hematuria. The opened bladder reveals masses of a neoplasm that histologically proved to be
transitional cell carcinoma (TCC). TCC can arise anywhere in the urothelium, but is most common in
bladder. TCC is often multifocal and has a tendency to recur.
Exophytic TCC of urinary bladder
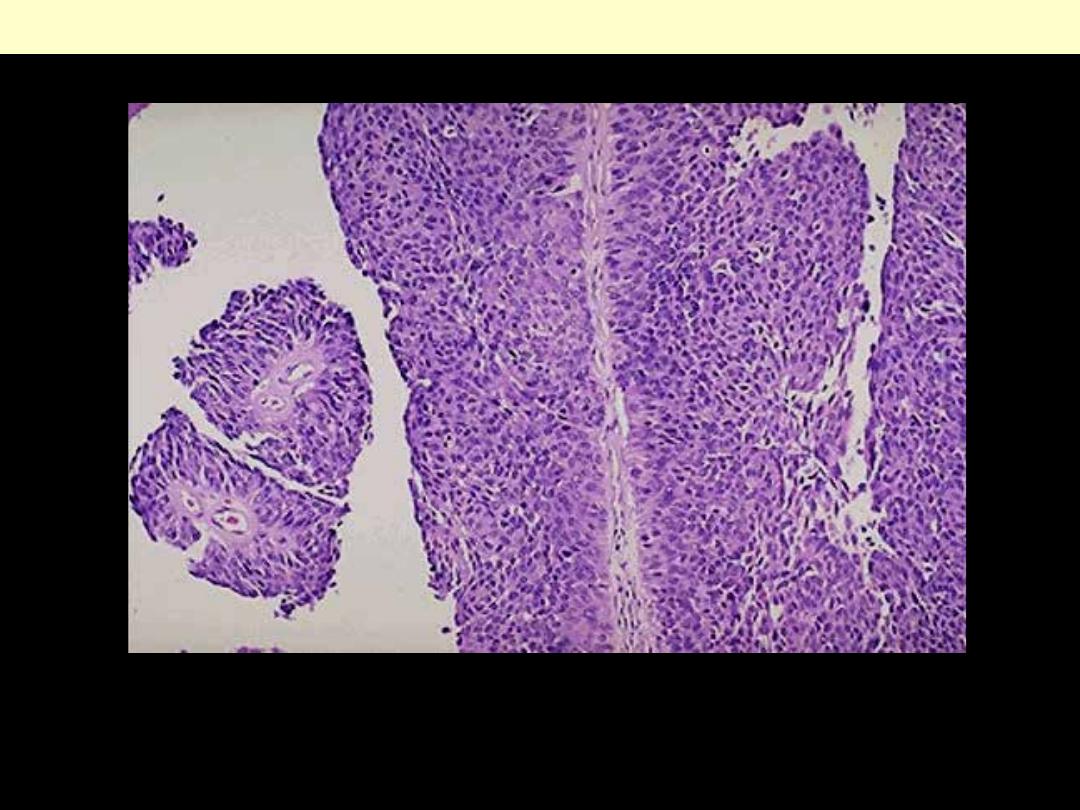
At high power, the transitional cell carcinoma does resemble urothelium, but the thickness is much
greater than normal and the cells show more pleomorphism.
Papillary TCC
The cut surface of the kidney removed surgically here demonstrate normal cortex and medulla, but the
calyces show focal papillary tumor masses of transitional cell carcinoma.
Papillary TCC of renal pelvis