Thoracic Trauma
TopicsIntroduction to Thoracic Trauma
Thoracic Anatomy
Pathophysiology of Thoracic Trauma
Assessment of Thoracic Trauma
Management of Thoracic Trauma
Chest Injuries
Directly responsible for more than 20% of all traumatic deaths (regardless of mechanism)
Account for about 16,000 deaths per year in the United States
Statistics
Chest injuries are the second leading cause of trauma deaths each year.Most thoracic injuries (90% of blunt trauma and 70% to 85% of penetrating trauma) can be managed without surgery.
Classifications of Chest Injuries
Skeletal injuryPulmonary injury
Heart and great vessel injury
Diaphragmatic injury
Mechanism of Injury:
Blunt thoracic injuries
Forces distributed over a large area
Deceleration
Compression
3-Penetrating thoracic injuries
Forces are distributed over a small area.
Organs injured are usually those that lie along the path of the penetrating object.
Injury Patterns:
General typesOpen injuries
Closed injuries
Cardiovascular
Pleural and pulmonary
Mediastinal
Diaphragmatic
Esophageal
Penetrating cardiac trauma
Blast injury
Confined spaces
Shock wave
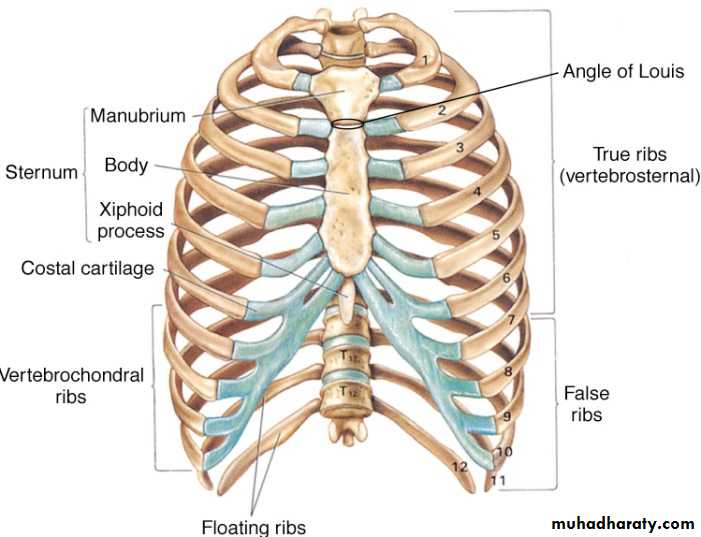
Thoracic cage
Anatomy
Skin
Bones
Thoracic cage
Sternum
Thoracic spine
Muscles
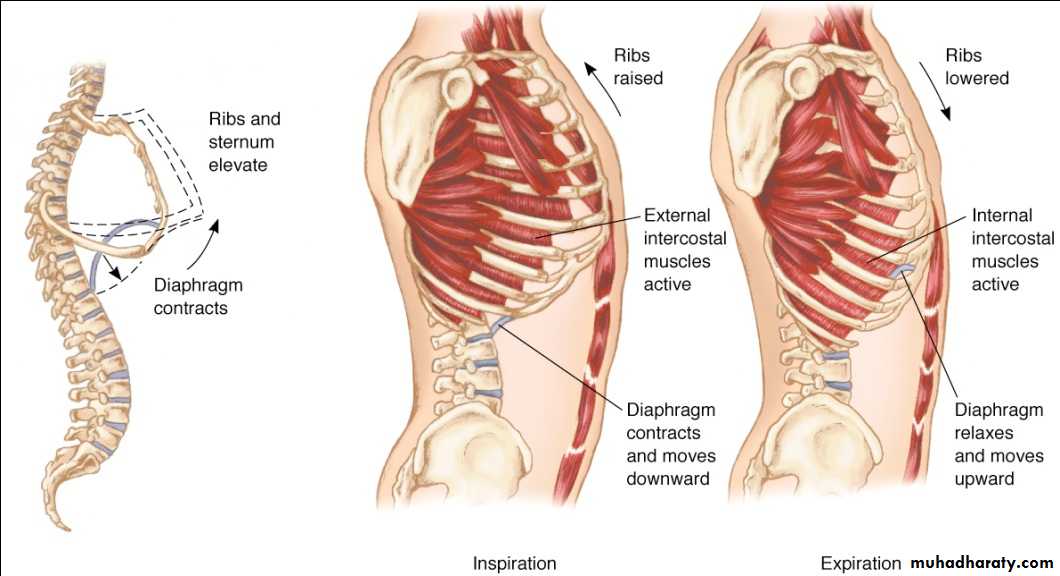
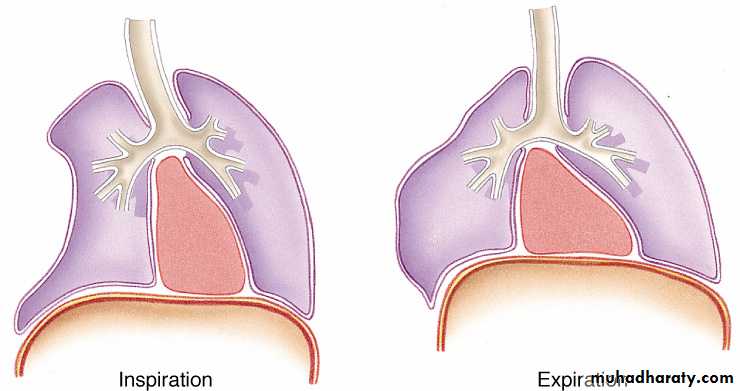
: The respiratory muscles contract in response to stimulation of the phrenic and intercostal nerves.
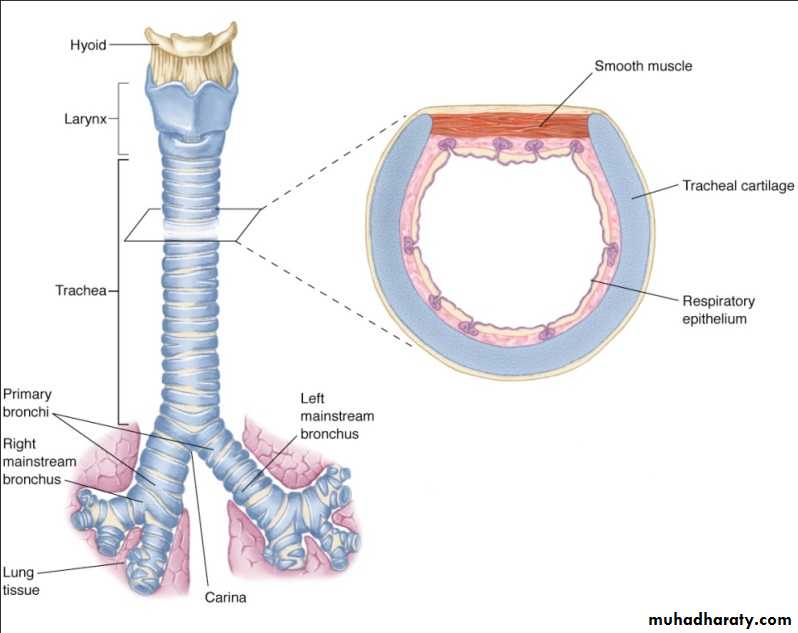
Trachea
Bronchi
Lungs
Vascular Anatomy
Arteries: Aorta, Carotid, Subclavian, Intercostal.
Veins: Superior vena cava ,Inferior vena cava ,Subclavian ,Internal jugular.
Pulmonary: Arteries ,Veins.
Heart: Ventricles ,Atria ,Valves ,Pericardium.
Anatomy
Mediastinum
The area between the lungs
Heart ,Trachea ,Vena cavae ,Pulmonary artery ,Aorta Esophagus
Lymph nodes.
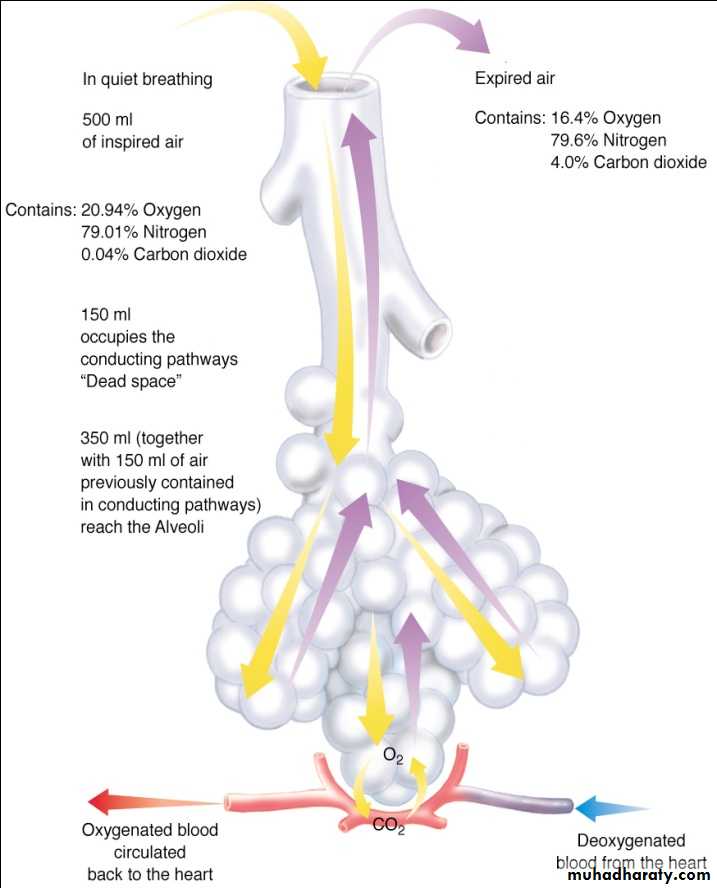
Physiology
Ventilation—the mechanical process of moving air into and out of the lungs
Respiration—the exchange of oxygen and carbon dioxide between the outside atmosphere and the cells of the body
Pathophysiology:
Impairments in cardiac outputBlood loss ,Increased intrapleural pressures ,Blood in the pericardial sac,
Myocardial valve damage ,Vascular disruption.
Impairments in gas exchange
Atelectasis ,Contused lung tissue ,Disruption of the respiratory tract.
Assessment Findings
PulseDeficit ,Tachycardia ,Bradycardia.
Blood pressure
Narrowed pulse pressure ,Hypertension ,Hypotension ,Pulsus paradoxus.
Respiratory rate and effort:
Tachypnea ,Bradypnea ,Labored ,Retractions ,Other evidence of respiratory distress
Skin
Diaphoresis,Pallor,Cyanosis,Open wounds, Ecchymosis,
Other evidence of trauma.
Assessment (Neck)
Position of trachea
Subcutaneous emphysema
Jugular venous distention
Penetrating wounds
Assessment (Chest)
Contusions
Tenderness
Asymmetry
Lung sounds:
Absent or decreased ,Unilateral ,Bilateral ,Location ,Bowel sounds in hemothorax.
Abnormal Percussion Finding
Hyperresonance–Air
Hyporesonance–Fluid
Assessment ECG
ST/T wave elevation or depression
Conduction disturbances
Rhythm disturbances
History
DyspneaChest pain
Associated symptoms
Other areas of pain or discomfort
Symptoms before incident
Past history of cardiorespiratory disease
Use of restraint in motor vehicle crash
Management
Airway and ventilationHigh-concentration oxygen
Pleural decompression
Endotracheal intubation
Needle cricothyrotomy
Surgical cricothyrotomy
Positive-pressure ventilation
Occlude open wounds
Stabilize chest wall
Circulation
Manage cardiac dysrhythmias
Intravenous access
Pharmacological: Analgesics, Antidysrhythmics
Nonpharmacological
Needle thoracostomy
Tube thoracostomy—in-hospital management
Pericardiocentesis—in-hospital management
Transport Considerations
Appropriate mode
Appropriate facility
Skeletal Injury
Clavicular fractures
Clavicle the most commonly fractured bone
Isolated fracture of the clavicle seldom a significant injury
Common causes
Children who fall on their shoulders or outstretched arms
Athletes involved in contact sports
Treatment
Usually accomplished with a sling and swathe or a clavicular strap that immobilizes the affected shoulder and arm
Usually heals well within 4 to 6 weeks
Signs and symptoms
Pain
Point tenderness
Evident deformity
Complications
Injury to the subclavian vein or artery from bony fragment penetration, producing a hematoma or venous thrombosis (rare)
Rib Fractures
IncidenceInfrequent until adult life
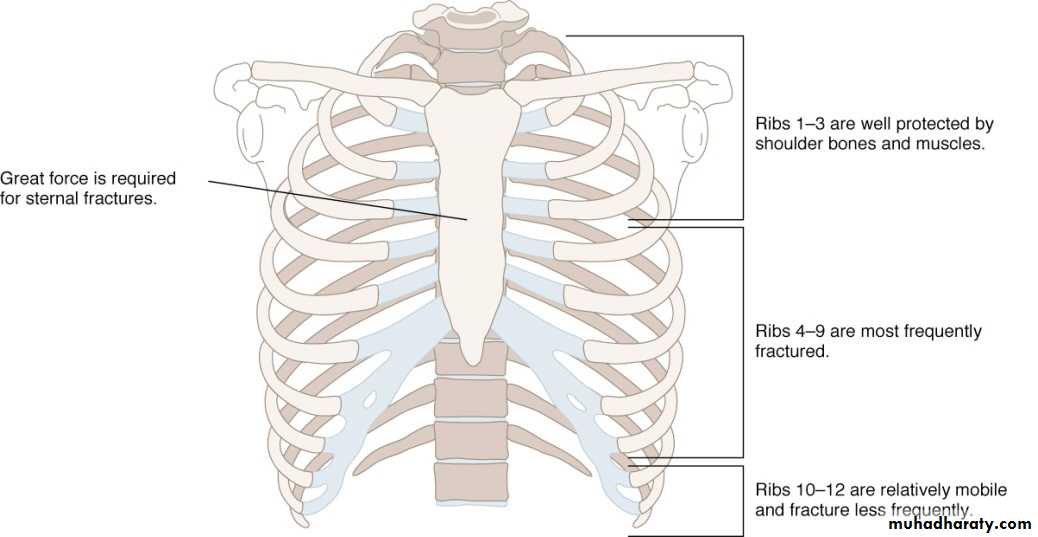
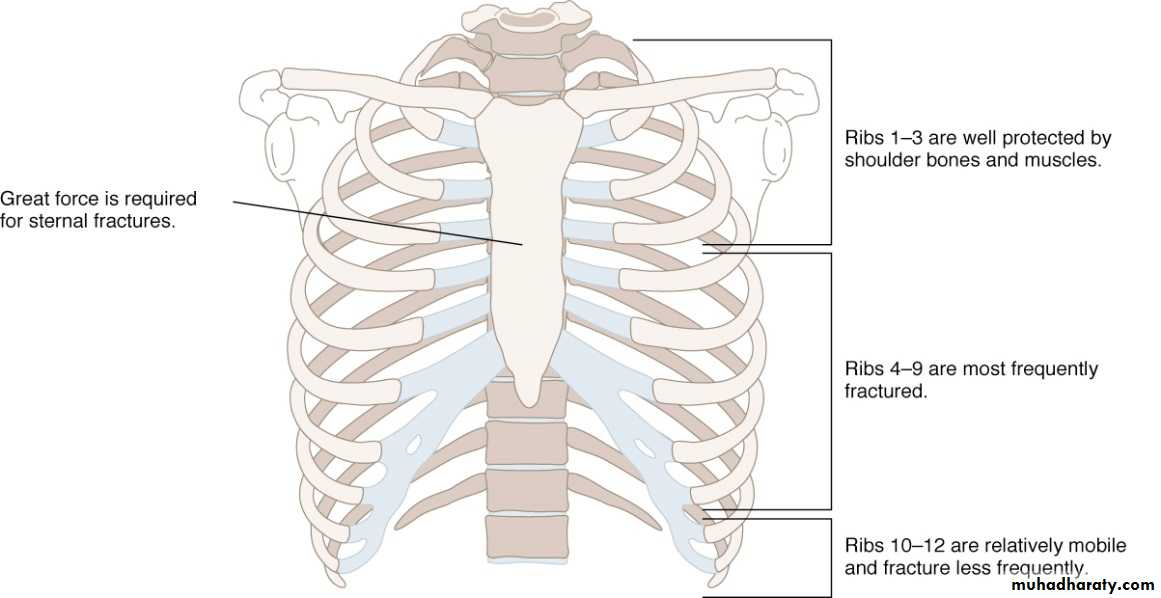
Significant force required
Most often elderly patients
Morbidity/Mortality
Can lead to serious consequences.
Older ribs are more brittle and rigid.
There may be associated underlying pulmonary or cardiovascular injury.
Pathophysiology
Most often caused by blunt trauma—bowing effect with midshaft fracture
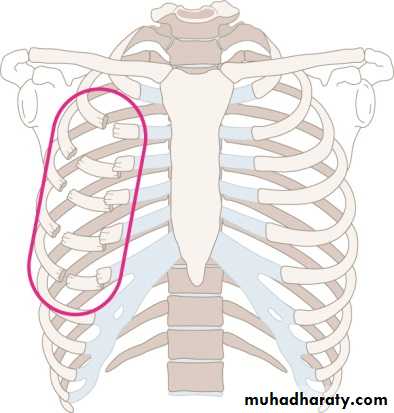
Ribs 3 to 8 are fractured most often (they are thin and poorly protected)
Respiratory restriction as a result of pain and splinting
Intercostal vessel injury
Associated complications
First and second ribs are injured by severe trauma
Rupture of the aorta
Tracheobronchial tree injury
Vascular injury
Multiple Rib Fractures
Atelectasis
Hypoventilation
Inadequate cough
Pneumonia
Assessment findings
Localized pain
Pain that worsens with movement, deep breathing, coughing
Point tenderness
Most patients can localize the fracture by pointing to the area (confirmed by palpation).
Crepitus or audible crunch
Splinting on respiration
Rib Fractures Complications
Splinting, which leads to atelectasis and ventilation-perfusion mismatch (ventilated alveoli that are not perfused or perfused alveoli that are not ventilated)
Rib Fractures Management
Airway and ventilationHigh-concentration oxygen
Positive-pressure ventilation
Encourage coughing and deep breathing
Pharmacological
Analgesics
Nonpharmacological
Non-circumferential splintingTransport Considerations
Appropriate mode
Appropriate facility
Flail Chest
Incidence: Most common cause: vehicular crash ,Falls from heights ,Industrial accidents ,Assault ,Birth trauma.Morbidity/Mortality
Significant chest trauma
Mortality rates 20% to 40% due to associated injuries
Mortality increased with
Advanced age ,7 or more rib fracture ,3 or more associated injuries ,Shock ,Head injuries.
Pathophysiology
Two or more adjacent ribs fractured in two or more places producing a free-floating segment of chest wallFlail chest usually results from direct impact.
Note:The flail segment classically involves anterior (sternal separation) or lateral rib fractures. Posterior rib fractures usually do not produce a flail segment because stability is provided by the heavy musculature.
Respiratory failure due to:
Underlying pulmonary contusion
The blunt force of the injury typically produces an underlying pulmonary contusion.
Associated intrathoracic injury
Inadequate bellows action of the chest
Assessment Findings
Chest wall contusion
Respiratory distress
Paradoxical chest wall movement
Pleuritic chest pain
Crepitus
Pain and splinting of affected side
Tachypnea
Tachycardia
Possible bundle branch block on ECG
Management
Airway and ventilation
High-concentration oxygen.
Positive-pressure ventilation may be needed.
Reverses the mechanism of paradoxical chest wall movement
Restores the tidal volume
Reduces the pain of chest wall movement
Assess for the development of a pneumothorax
Evaluate the need for endotracheal intubation.
Stabilize the flail segment (controversial).
Note:In the presence of underlying lung or chest injury, positive-pressure ventilation may promote the development of a pneumothorax because of delayed exhalation and increased intrapulmonic pressures.
Sternal Fractures
IncidenceOccurs in 5% to 8% of all patients with blunt chest trauma
A deceleration compression injury - Steering wheel - Dashboard
A blow to the chest; massive crush injury - Severe hyperflexion of the thoracic cage
Morbidity/Mortality
25% to 45% mortality rate
High association with myocardial or lung injury:
Myocardial contusion ,Myocardial rupture ,Cardiac tamponade, Pulmonary contusion.
Pathophysiology
Associated injuries cause morbidity and mortality.
Pulmonary and myocardial contusion
Flail chest
Seriously displaced sternal fractures may produce a flail chest.
Vascular disruption of thoracic vessels
Intra-abdominal injuries
Head injuries
Management
Airway and ventilation: High-concentration oxygen
Circulation: restrict fluids if pulmonary contusion suspected
Pharmacological—analgesics
Nonpharmacological—allow chest wall self-splinting
Transport considerations: - Appropriate mode - Appropriate facility
Psychological support/communication strategies
Pulmonary Injury
Closed (simple) pneumothorax
Incidence
10% to 30% in blunt chest trauma
Almost 100% with penetrating chest trauma
Morbidity/mortality
Extent of atelectasis
Associated injuries
Pathophysiology
Caused by the presence of air in the pleural space
A common cause of pneumothorax is a fractured rib that penetrates the underlying lung.
May occur in the absence of rib fractures from:
A sudden increase in intrathoracic pressure generated when the chest wall is compressed against a closed glottis (the paper-bag effect)
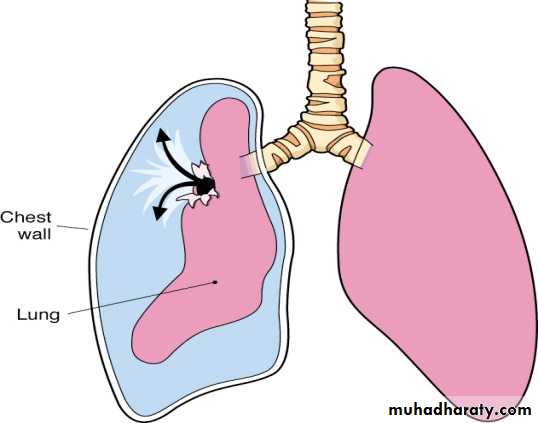
Results in an increase in airway pressure and ruptured alveoli, which lead to a pneumothorax
Small tears self-seal; larger ones may progress.
The trachea may tug toward the affected side.
Ventilation/perfusion mismatch.
Assessment Findings
TachypneaTachycardia
Respiratory distress
Absent or decreased breath sounds on the affected side
Hyperresonance
Decreased chest wall movement
Dyspnea
Chest pain referred to the shoulder or arm on the affected side
Slight pleuritic chest pain
Management
Airway and ventilation
High-concentration oxygen.
Positive-pressure ventilation if necessary.
If respiration rate is <12 or >28 per minute, ventilatory assistance with a bag-valve mask may be indicated.
Nonpharmacological: Needle thoracostomy
Transport considerations
Position of comfort (usually partially sitting) unless contraindicated by possible spine injury
Appropriate mode
Appropriate facility

Open Pneumothorax
Incidence
Usually the result of penetrating trauma: - Gunshot wounds - Knife wounds - Impaled objects - Motor vehicle collisions - Falls
Morbidity/Mortality
Severity is directly proportional to the size of the wound.
Profound hypoventilation can result.
Death is related to delayed management.
Pathophysiology
An open defect in the chest wall (>3 cm)
If the chest wound opening is greater than two-thirds the diameter of the trachea, air follows the path of least resistance through the chest wall with each inspiration.
As the air accumulates in the pleural space, the lung on the injured side collapses and begins to shift toward the uninjured side.
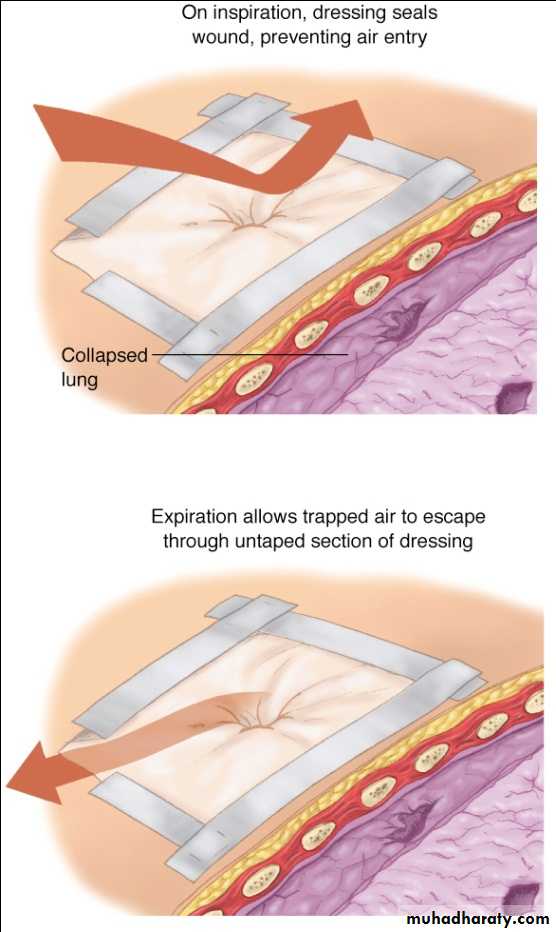
Very little air enters the tracheobronchial tree to be exchanged with intrapulmonary air on the affected side, which results in decreased alveolar ventilation and decreased perfusion.
The normal side also is adversely affected because expired air may enter the lung on the collapsed side, only to be rebreathed into the functioning lung with the next ventilation.
May result in severe ventilatory dysfunction, hypoxemia, and death unless rapidly recognized and corrected.Assessment Findings
To-and-fro air motion out of the defect
A defect in the chest wall
A penetrating injury to the chest that does not seal itself
A sucking sound on inhalation
Tachycardia
Tachypnea
Respiratory distress
Subcutaneous emphysema
Decreased breath sounds on the affected side
Management
Airway and ventilation:
High-concentration oxygen.
Positive-pressure ventilation if necessary.
Assist ventilations with a bag-valve device and intubation as necessary.
Monitor for the development of a tension pneumothorax.
Circulation—treat for shock with crystalloid infusion.
Nonpharmacological: Occlude the open wound—apply an occlusive petroleum gauze dressing (covered with sterile dressings) and secure it with tape.
Tension Pneumothorax
Associated Injuries
A penetrating injury to the chest
Blunt trauma
Penetration by a rib fracture
Many other mechanisms of injuryMorbidity/Mortality
Profound hypoventilation can result.
Death is related to delayed management.
An immediate, life-threatening chest injury.
Pathophysiology
Occurs when air enters the pleural space from a lung injury or through the chest wall without a means of exit.Results in death if it is not immediately recognized and treated.
When air is allowed to leak into the pleural space during inspiration and becomes trapped during exhalation, an increase in the pleural pressure results.
Increased pleural pressure produces mediastinal shift.
Mediastinal shift results in:
Compression of the uninjured lung
Kinking of the superior and inferior vena cava, decreasing venous return to the heart, and subsequently decreasing cardiac output
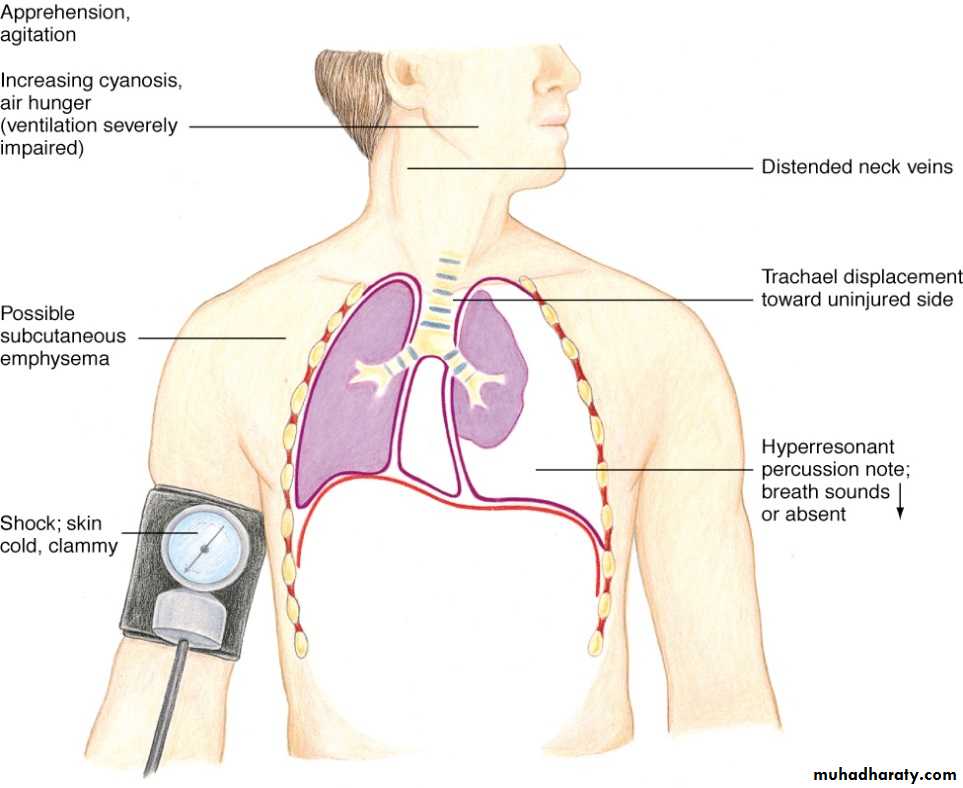
Assessment Findings
Extreme anxiety
Cyanosis
Increasing dyspnea
Difficult ventilations while being assisted
Tracheal deviation (a late sign)
Hypotension
Identification is the most difficult aspect of field care in a tension pneumothorax.
Tachycardia
Diminished or absent breath sounds on the injured side
Tachypnea
Respiratory distress
Bulging of the intercostal muscles
Subcutaneous emphysema
Jugular venous distention (unless hypovolemic)
Unequal expansion of the chest (tension does not fall with respiration)
Hyperresonnace to percussion
Physical Findings
Management
Emergency care is directed at reducing the pressure in the pleural space.Airway and ventilation:
High-concentration oxygen
Positive pressure ventilation if necessary
Circulation—relieve the tension pneumothorax to improve cardiac output.
Nonpharmacological
Occlude open wound
Needle thoracostomy
Tube thoracostomy—in-hospital management
Pleural decompression should only be employed if the patient demonstrates significant dyspnea and distinct signs and symptoms of tension pneumothorax.
Needle thoracostomy
Tension pneumothorax associated with penetrating trauma
May occur when an open pneumothorax has been sealed with an occlusive dressing.
Pressure may be relieved by momentarily removing the dressing (air escapes with an audible release of air).
After the pressure is released, the wound should be resealed.
Tension pneumothorax associated with closed trauma
If the patient demonstrates significant dyspnea and distinct signs and symptoms of tension pneumothorax:
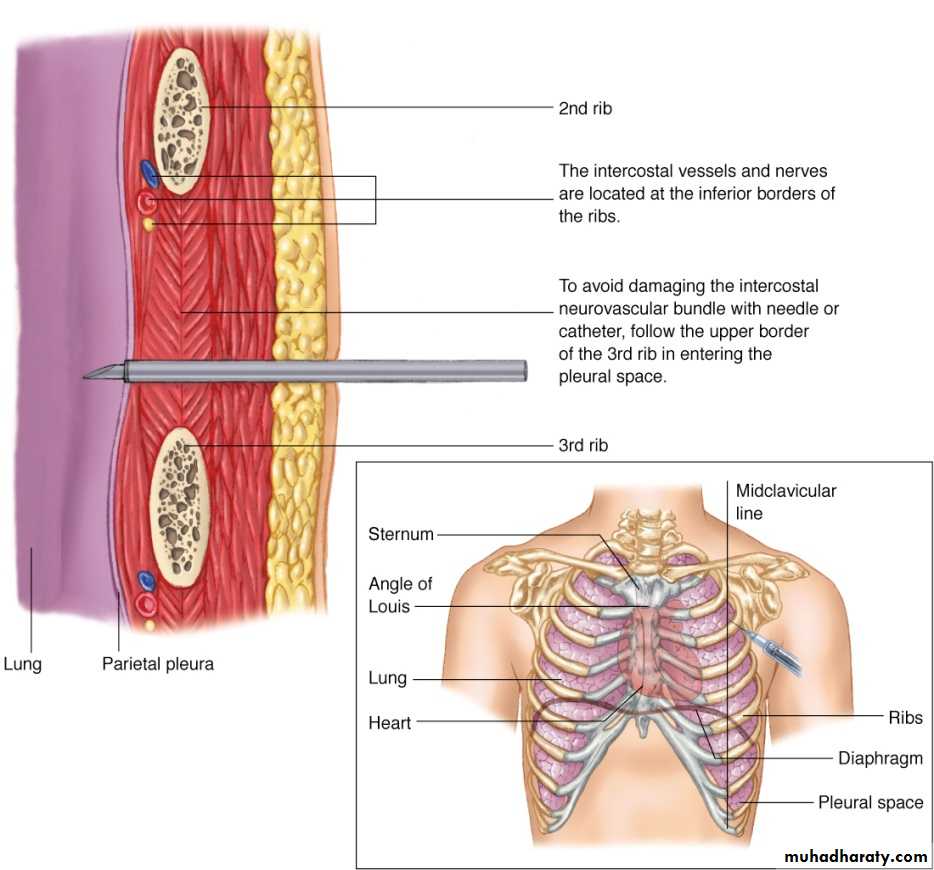
Provide thoracic decompression with either a large-bore needle or commercially available thoracic decompression kit.
Insert a 2-inch 14- or 16-gauge hollow needle or catheter into the affected pleural space.
Usually the second intercostal space in the midclavicular line
Insert the needle just above the third rib to avoid the nerve, artery, and vein that lie just beneath each rib.
Hemothorax
If this condition is associated with pneumothorax, it is called a hemo- pneumothorax.Incidence
Associated with pneumothorax.
Blunt or penetrating trauma.
Rib fractures are frequent cause.
Morbidity/Mortality
A life-threatening injury that frequently requires urgent chest tube placement and/or surgery
Associated with great vessel or cardiac injury
50% of these patients will die immediately.
25% of these patients live 5 to 10 minutes.
25% of these patients may live 30 minutes or longer.
Pathophysiology
Accumulation of blood in the pleural space caused by bleeding from
Penetrating or blunt lung injury
Chest wall vessels
Intercostal vessels
Myocardium
Hypovolemia results as blood accumulates in the pleural space.
Assessment Findings
Tachypnea ,Dyspnea
Cyanosis
Often not evident in hemorrhagic shock
Diminished or decreased breath sounds on the affected side
Hyporesonance (dullness on percussion) on the affected side
Hypotension
Narrowed pulse pressure
Tracheal deviation to the unaffected side (rare)
Pale, cool, moist skin

Physical Findings
ManagementAirway and ventilation
High-concentration oxygen
Positive-pressure ventilation if necessary
Ventilatory support with bag-valve mask, intubation, or both
Circulation
Administer volume-expanding fluids to correct hypovolemia
Nonpharmacological—tube thoracostomy (in-hospital management)
Transport considerations
Appropriate mode
Appropriate facility
Hemopneumothorax
Pathophysiology—pneumothorax with bleeding in the pleural spaceAssessment—findings and management are the same as for hemothorax.
Management—management is the same as for hemothorax.
Pulmonary Contusion
A pulmonary contusion is the most common potentially lethal chest injury.Incidence
Blunt trauma to the chest
The most common injury from blunt thoracic trauma.
30% to 75% of patients with blunt trauma have pulmonary contusion.
Commonly associated with rib fracture
High-energy shock waves from explosion
High-velocity missile wounds
Rapid deceleration
A high incidence of extrathoracic injuries
Low velocity—ice pickMorbidity/Mortality
May be missed due to the high incidence of other associated injuries
Pulmonary Contusion
Mortality—between 14% and 20%
Assessment Findings
Tachypnea ,Tachycardia ,Cough ,Hemoptysis ,Apprehension ,Respiratory distress ,Dyspnea ,Evidence of blunt chest trauma ,Cyanosis.Management
Airway and ventilation:
High-concentration oxygen
Positive-pressure ventilation if necessary
Circulation—restrict IV fluids (use caution restricting fluids in hypovolemic patients).
Transport considerations.
Traumatic Asphyxia
Incidence
A severe crushing injury to the chest and abdomen
Steering wheel injury
Conveyor belt injury
Compression of the chest under a heavy object
Pathophysiology
A sudden compressional force squeezes the chest.
An increase in intrathoracic pressure forces blood from the right side of the heart into the veins of the upper thorax, neck, and face.
Jugular veins engorge and capillaries rupture.
Assessment:
Reddish-purple discoloration of the face and neck (the skin below the face and neck remains pink).Jugular vein distention.
Swelling of the lips and tongue.
Swelling of the head and neck.
Swelling or hemorrhage of the conjunctiva (subconjunctival petechiae may appear).
Hypotension results once the pressure is released.
Management
Airway and ventilation
Ensure an open airway ,Provide adequate ventilation.
Circulation
IV access.
Expect hypotension and shock once the compression is released.
Transport considerations
Appropriate mode.
Appropriate facility.