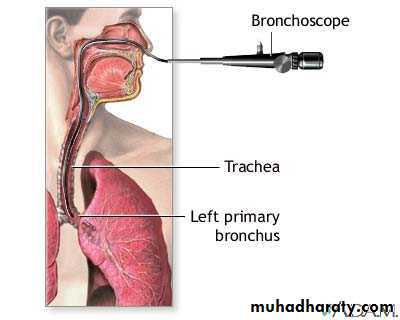
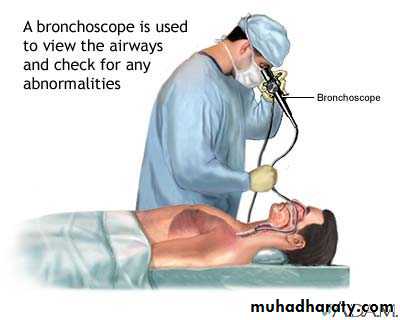
Bronchoscopy
Bronchoscopy Looking into the living lungs (Chevalier Jackson 1928)Today with the major advance in technology View the fine details of the end bronchial anatomy Diagnosis of the disease Treating diseases It is the visualization of the air way using either rigid Bronchoscope (GA) or the flexible (Fiber optic Bronchoscope ) (LA) or both simultaneously .Through which we can remove FB , take BAL , brushing lesions &Trans bronchial Biopsy .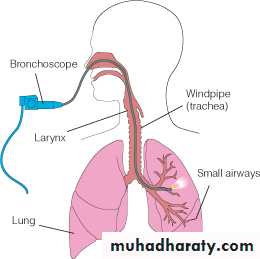
HISTORY
• Gustav Killian in 1897 succeeded in removing aspirated pork bone from the bronchus of a 63 –year-old farmer under cocaine anesthesia .He used external light source , a head mirror , esophagoscope and forceps to remove the bone .• He became famous & his clinic attracted patients from far and wide for his expertise in removing different kind of (FB) such as bones ,beans ,buttons ,coins & tin whistle .
Gustav Killian (The father of bronchoscopy ) , was appointed professor
of ENT at the university of Freiburg in 1892 .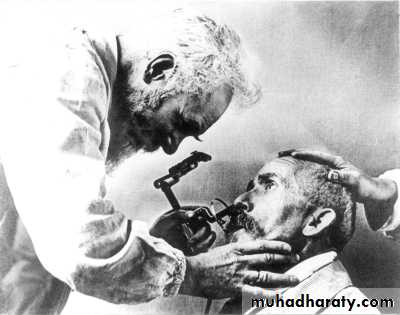
Gustav Killian Bronchoscope , external light source
Bronchoscopy rapidly developed into a science (with the creation of a better instruments and techniques )Chevalier Jackson Founded philadelphia school of bronchoesophagology Jackson‘s monograph first published in 1950
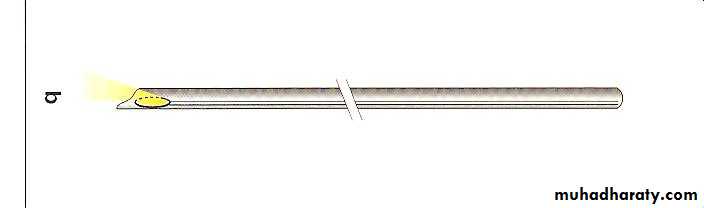
Chevalier Jackson’s Bronchoscope with a small distal bulb & built –in suction tube
• H.H.Hopkins English physicist developed the rod-lens optical telescopes which could be used with the rigid bronchoscope
Early in the 1960s Shigeto Ikeda devised a means to replace the small electric bulb with glass fibers capable of transmitting brighter light from an outside source. He presented the first flexible bronchoscope at the 1966 International Congress on Diseases of the Chest in Copenhagen.

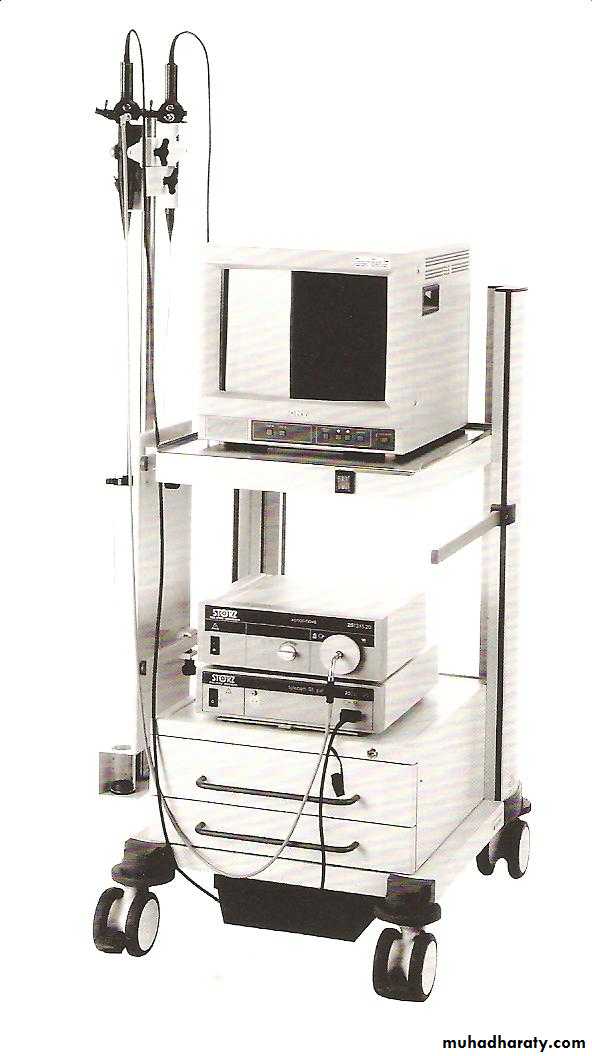
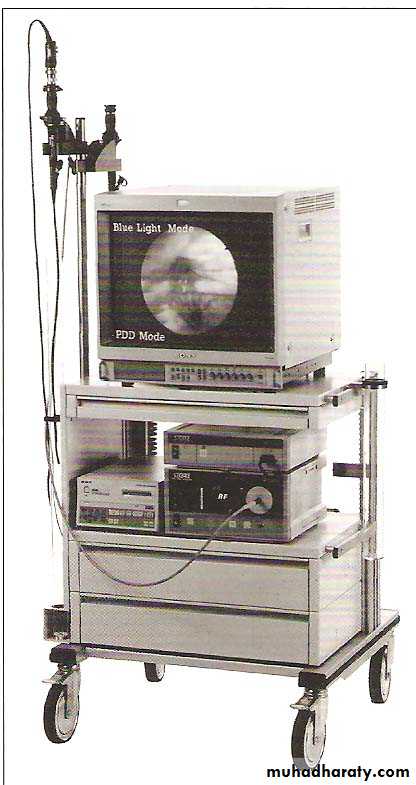
At the end of the 1980s, Asahi Pentax replaced the fiberoptic bundle with a charge-coupled sensor at the tip of the scope. This videobronchoscope allowed the bronchoscopist to look at a monitor screen instead of through the eyepiece of the scope

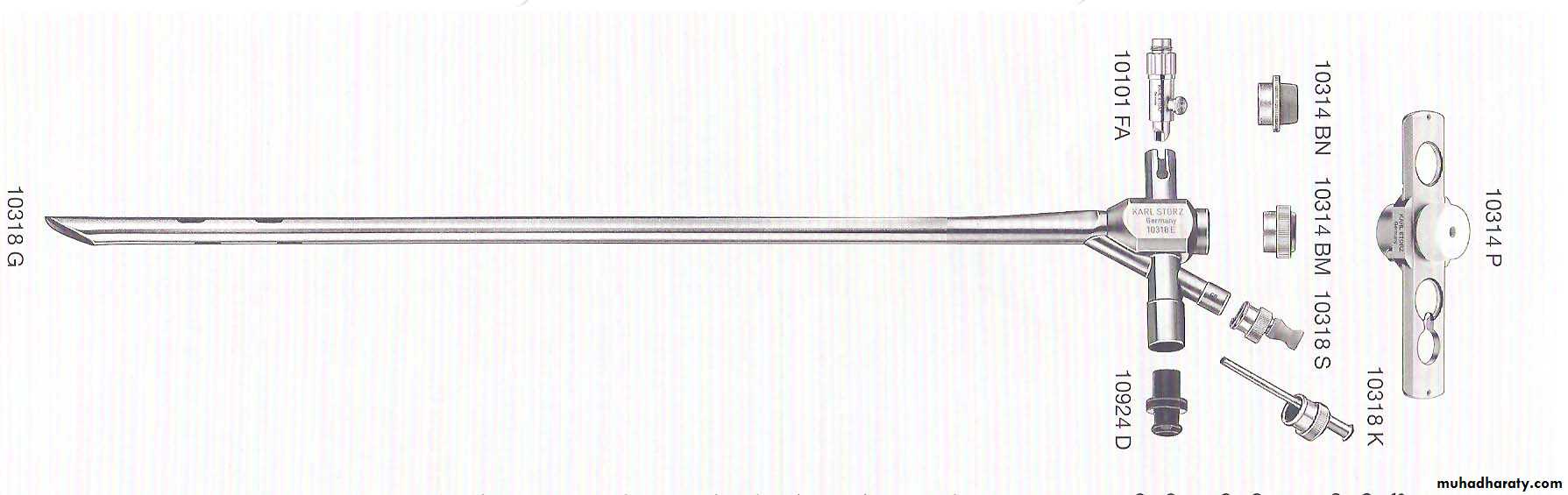
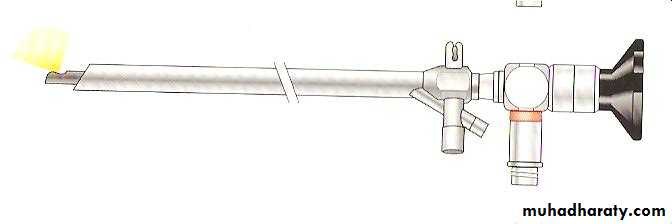
Rigid Bronchoscopes
• Hollow metal tubes , of variables sizes down to ( 3mm -9.5 mm) and variable length (20-40 cm) .These instruments usually have illumination at their tips as well as side holes near the tip to facilitate ventilation .They are always inserted trans orally .General anesthesia is recommended for its introduction .• i.e. Diagnostic and Therapeutic
• Indications for Rigid Bronchoscopy
• 1-Hemoptysis
• 2-Tracheal stenosis.
• 3-Foreign body removal .
• 4-All bronchological interventions such as bougienage , removal of threads & post intervention hemoptysis.
• 5-Confirmation of cell type in case of previous , non diagnostic fiberoptic bronchoscopy .
• 6-Laser treatment
• 7-Removal of tumor
• 8-Removal of excess fibrin , mucous plug .
• 9-Bronchography .
• 10-Autofluorescence and photodynamic diagnosis .
• Endoscopey for the museum

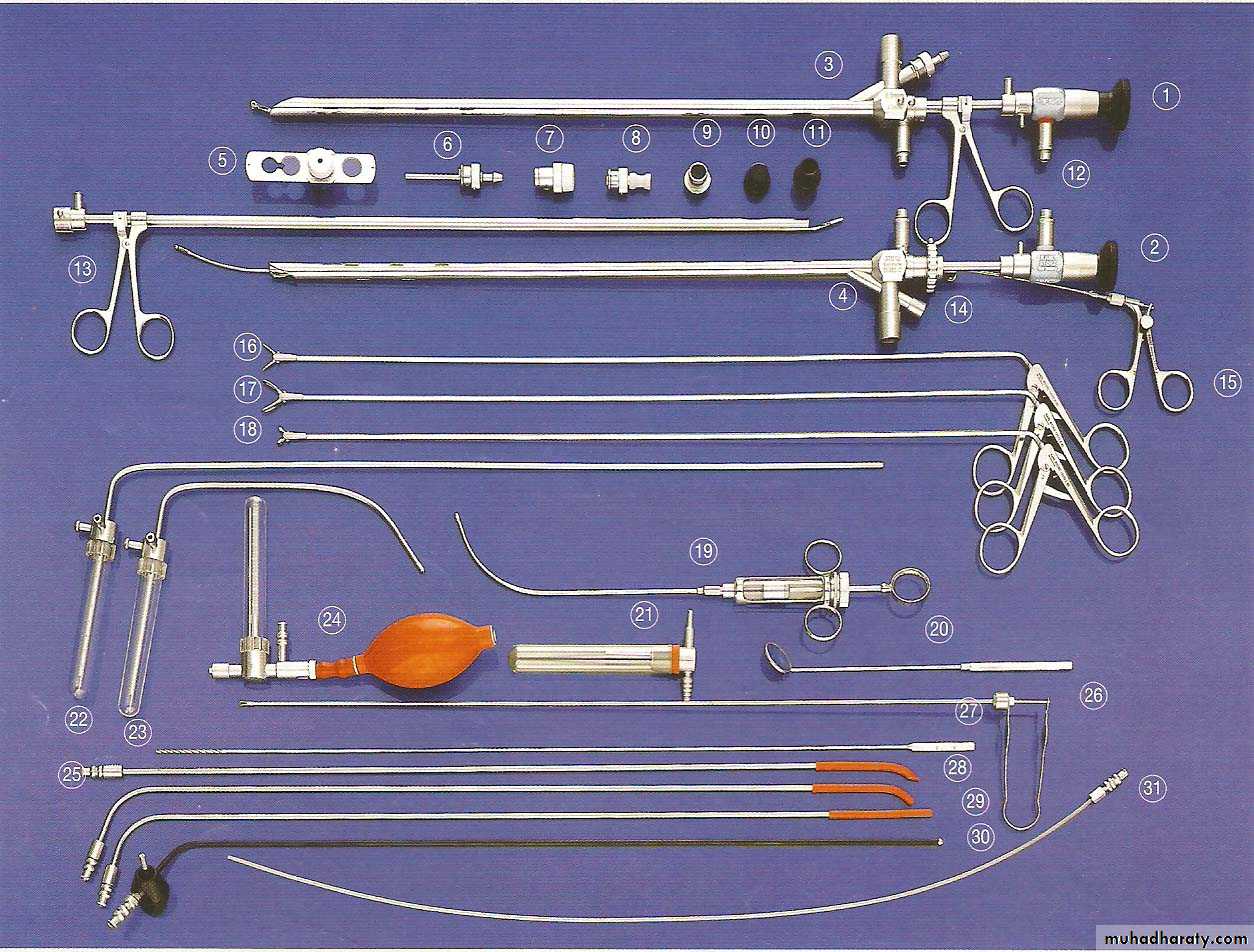
Bronchoscopy ( Adult Set )
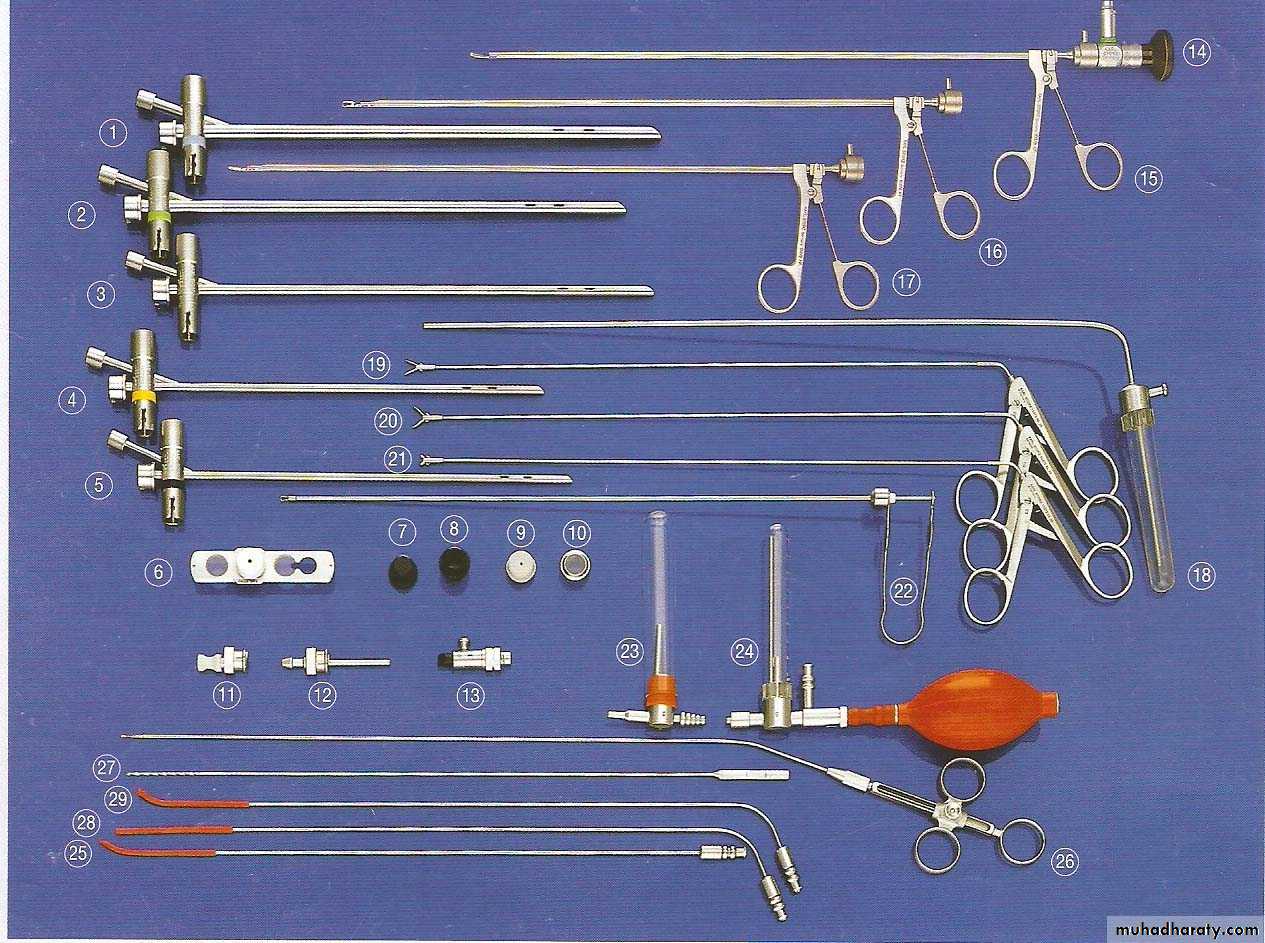
Bronchoscopy (Pediatric Set )
•




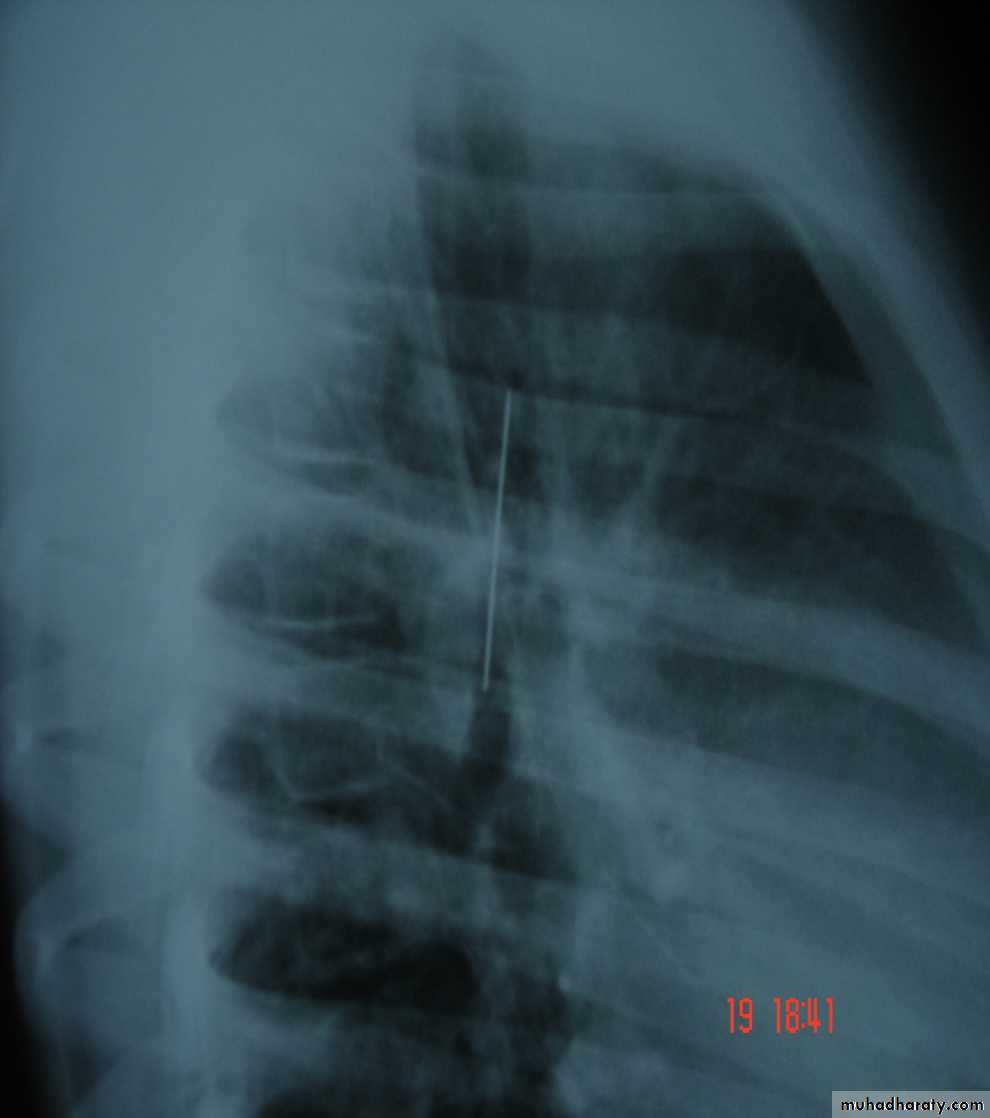
Foreign Body (RMB)
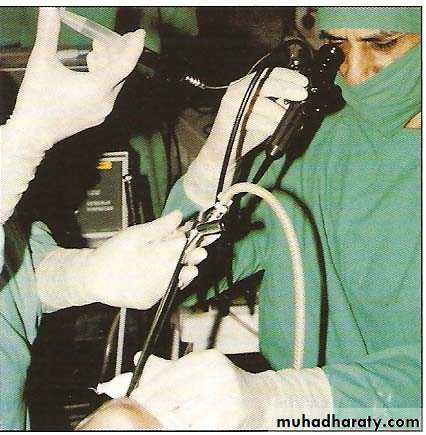
Flexible Bronchoscopy
It consists of Control section , a flexible insertion tube & a bending tip .The control section contains the eye piece ,control lever and a channel for aspiration or for introduction of solution and instruments.
• These flexible bronchoscopes have variable outside diameter (1.8 -6 mm) with inner channel ranging from (1.8 -2.6 mm) . Highly maneuverable and can reach areas in the endo bronchial tree not accessible to the rigid bronchoscopes .Can be inserted either transorally or transnasally or through the rigid bronchoscope.We have the Infantile , Pediatric , adult types and the Video –Bronchoscopes

• Major disadvantage of the flexible Bronchoscope is that it is a closed system that does not provide an airway , and the relatively small inner channel is considered to be incapable of allowing adequate suction when confronted with copious secretions or massive haemoptysis .
• It is not so much effective in the removal of foreign bodies .
Indications for flexible Bronchoscopy
1-For routine examinations .
2-Treatment of acute respiratory problems in the ICU.
3-Suction under visual control .
4-Use of catheter and brushes for cytology.
5-For obtaining secretions for bacteriological tests.
6-Localization of the bleeding site in case of hemoptysis.
7-Theraputic suction & irrigation .
8-Transbronchial lung biopsy .
9-Selective bronchography .
10-Autofluorescence & photodynamic diagnosis .
•
Tracheo-Bronchial Trainer

Sample collection (BAL)
Saline for irrigationLever
SuctionLecture scope
Rigid Bronchoscopy Is best avoided in the presence of Cervical spine injury thoracicto prevent hyperextension of the neck & in patient with Aneurysm of the aorta• Flexible Bronchoscopy
• Best avoided in patient with Massive Haemoptysis & patients with air way problems
Contra indications
In cases of doubt as to whether bronchoscopy should be done or not , bronchoscopy should always be done ( Jackson’s 1915 statement ) .
In suspected cases of F.B inhalation it is better to have a negative bronchoscopy rather than to miss a F.B inside with all its pathological consequences .
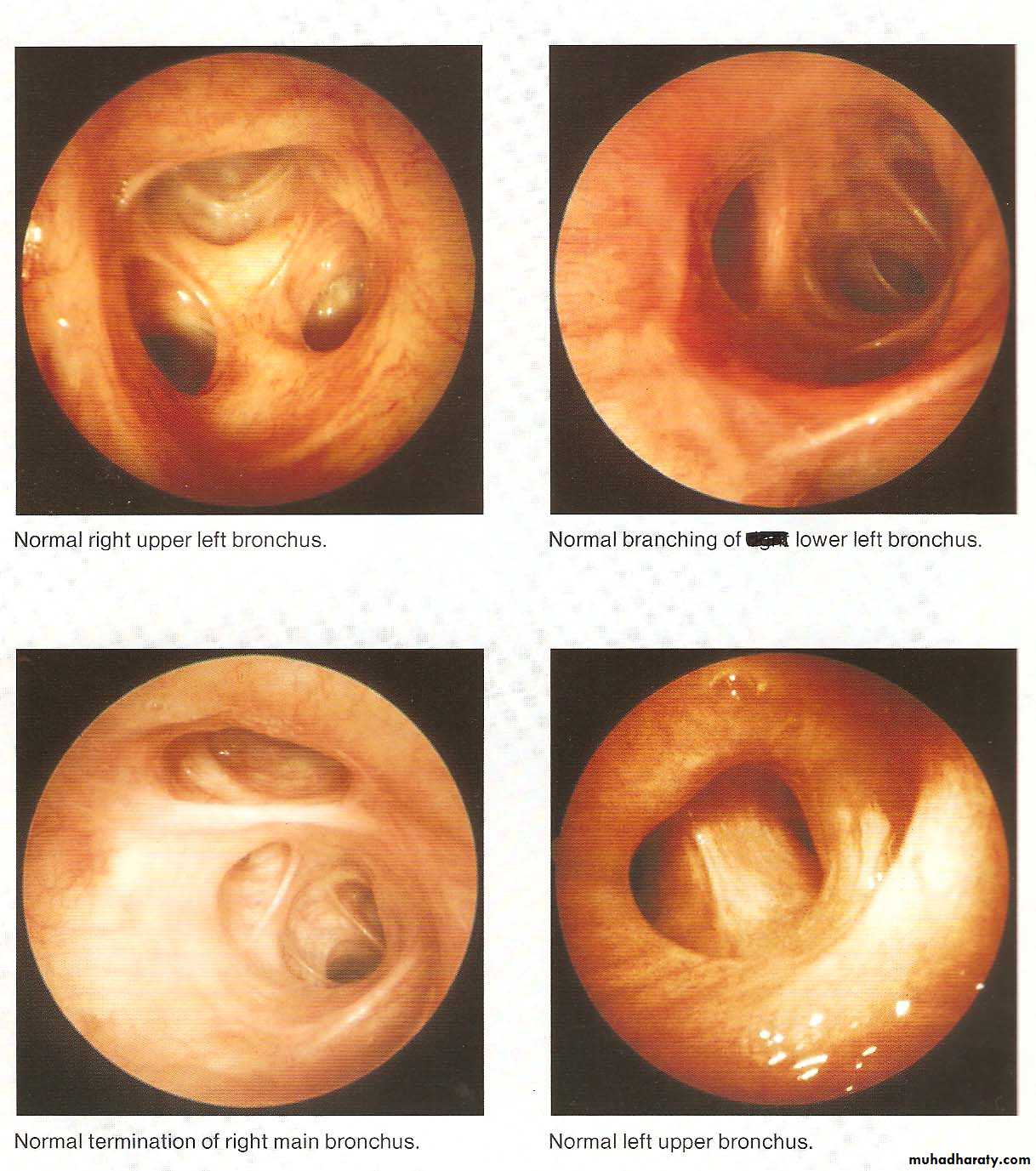
• Normal Bronchoscopic Findings
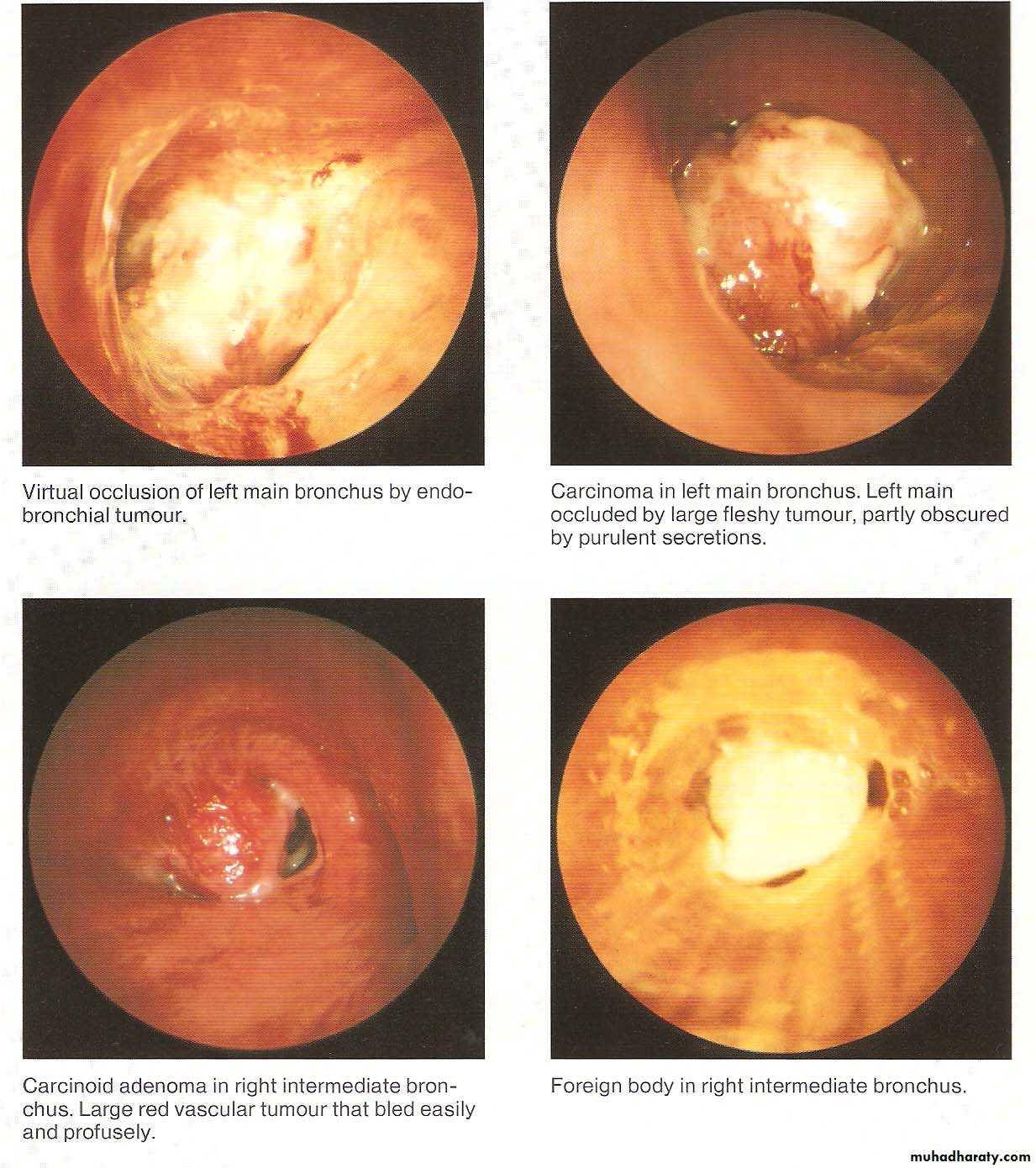
• Abnormal Bronchoscopic Findings
• COMPLICATIONS
• When bronchoscopy performed by properly trained individuals• It is a safe procedure .However a variety of other problems have been reported including
• Pneumothorax , bronchospasm , Bronchial perforation (Surgical emphysema & tension pneumothorax ) ,
• Subglottic edema , Uncontrolled bleeding , Infections
• Arrhythmias rarely ( Cardiopulmonary arrest )
• Hypoventilation (Hypoxia& hypercapnia)
• Majority related to a biopsy procedure So explorative thoracotomy may be safer than (injudicious biopsy )
• Some minor complications
• Damage of teeth , Injuries to lips or mouth
• Post bronchoscopy care
• 1-Close monitoring for 2-4 hours after the procedure
• 2-Eating and drinking is not allowed until the effect of anesthesia have worn off .
• 3-Some may advise routine CXR after performing a biopsy to check for signs of pneumothorax .
• 3-Those patients develop complications may need to stay in the hospital for additional time .
• 4-The patients may have sore throat , hoarseness ,cough or muscle ache .
• Fever up to temperature 38 “ c is common after bronchoscopy but usually for only 24 hours .
• Advances in Bronchoscopy
• 1- Brochoscopic Ultra-sound• 2-Bronchoscopic stenting (Air way prosthesis )
• 3-PDD & AF Bronchoscopy .
• 4-Bronchoscopic Laser therapy .
• 5-Bronchoscopic Electro Cautery
• 6-Cryo therapy
• 7-Brachy therapy
• 8-Photo therapy
Bronchoscopy need cooperation and mutual understanding Between
1-A well trained endoscopist2-a qualified staff
3-Expert and well trained anesthetist
Bronchoscopy
is now an integral part of respiratory medicine.
Diagnostic indications include tissue diagnosis, detection and staging of lung malignancy, evaluation of diffuse lung diseases like sarcoidosis and idiopathic interstitial pneumonias, pulmonary inspection of burn patients, identification of organisms infecting the respiratory tract and lungs.
As a therapeutic modality, bronchoscopy is used to place stents to protect airways vulnerable to collapse or occlusion, to remove foreign bodies or masses, to treat early stage endobronchial malignancy.