TRACHEAL & BRONCHIAL DISEASES
Benign Tumors of Trachea and BronchiAre rare ,more in males .They are slowly growing .Their presentation is is as a result of luminal obstruction or mucosal irritation .Patients may present with dyspnea , cough and haemoptysis .A sub glottic tumor presents with stridor ,The diagnosis is by bronchoscopy and treatment is surgical excision .E.g Papilloma , Haemangioma ,Chondroma and Fibroma.
Bronchial Adenomas
1-Bronchial Carcinod2-Muco epidermoid Tumors
3-Adenoid Cystic Carcinomas (Cylindromas )
4-Mucous Gland Adenomas
The first three are potentially malignant ,the 4th. Is benign
The first three are slowly growing , invade locally and surgical excision is the treatment of choice .
Bronchial Carcinoid Tumors
Resemble intestinal carcinoid as the cytoplasm as the cytoplasm of their cells contains neurosecretory granules .In the bronchus these tumors arise from the neuro endocrine argentafin cells of bronchial mucosa (Kultchitsky ‘s cells ) .They are grouped among APUD tumors (Amine Percursor Uptake Decaboxylation) .
They are capable of producing a number of hormones like Serotonin , histamine and gastrin .They are slowly growing tumors , but sometime they are aggresaive termed (atypical carcinoid ) .They present with cough , haemoptysis and dyspnea ) .
Carcinoid Syndrome is a rare ,presents with episodes of flushing , diarrhea and in addition to the systemic manifestations ,there may be cardiac manifestations .Elavated 5-HIAA may be detected in the urine ,which may be diagnostic .Bronchoscopic appearance is diagnostic and severe bleeding may follow a biopsy .Surgical excision is the treatment of choice .
Bronchial Carcinoid Tumors
Resemble intestinal carcinoid as the cytoplasm as the cytoplasm of their cells contains neurosecretory granules .In the bronchus these tumors arise from the neuro endocrine argentafin cells of bronchial mucosa (Kultchitsky ‘s cells ) .They are grouped among APUD tumors (Amine Percursor Uptake Decaboxylation) .
They are capable of producing a number of hormones like Serotonin , histamine and gastrin .They are slowly growing tumors , but sometime they are aggresaive termed (atypical carcinoid ) .They present with cough , haemoptysis and dyspnea ) .
Carcinoid Syndrome is a rare ,presents with episodes of flushing , diarrhea and in addition to the systemic manifestations ,there may be cardiac manifestations .Elavated 5-HIAA may be detected in the urine ,which may be diagnostic .Bronchoscopic appearance is diagnostic and severe bleeding may follow a biopsy .Surgical excision is the treatment of choice .
• Carcinoma of the lung
• Affects both sexes , It is however commoner in men It has poor prognosis .
• The incidence has shown a marked rise during recent years partly because of improved methods of diagnosis and partly due to• 1-Excessive cigarette smoking ,both active & passive smoking are implicated
• 2-Inhalation of irritants , such as silica &cobalt dust .


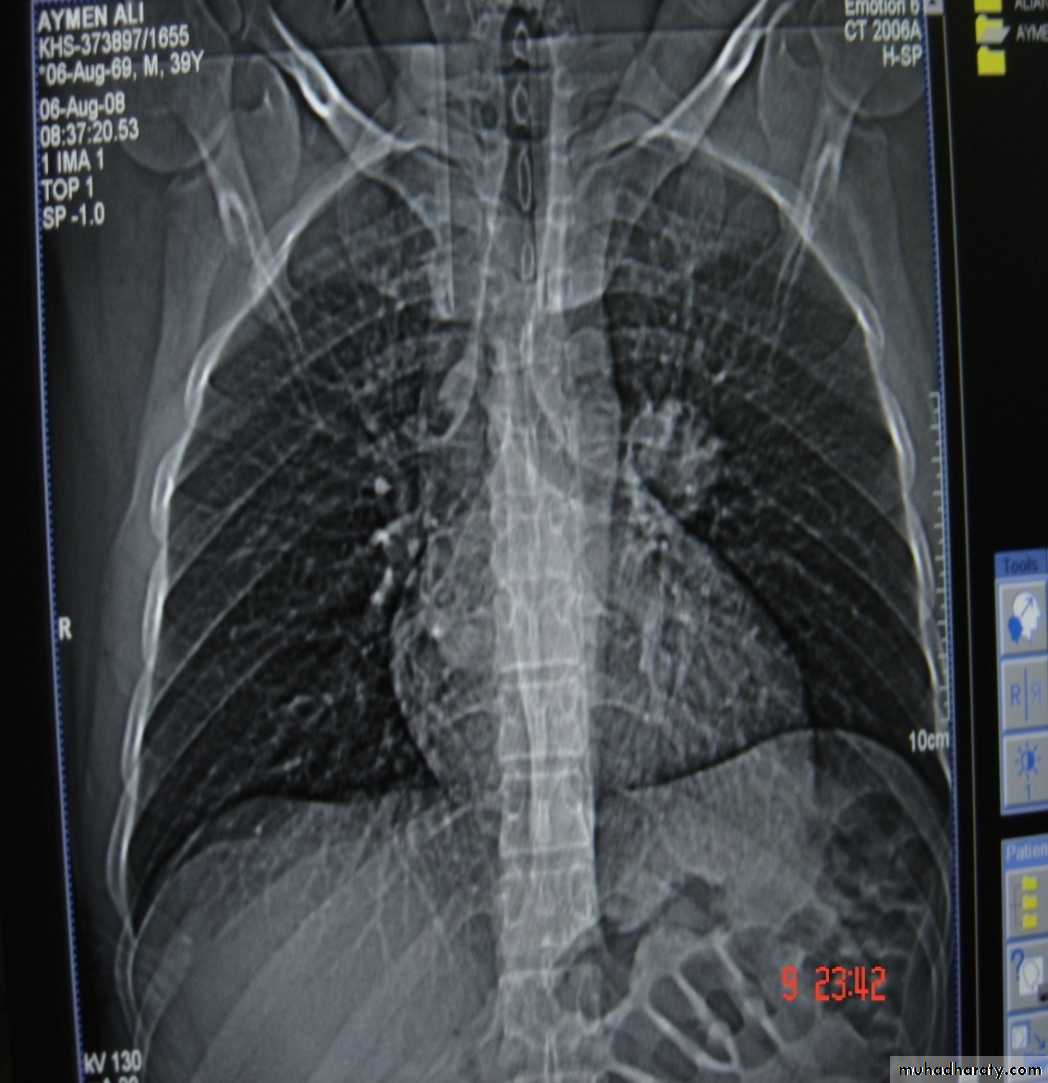
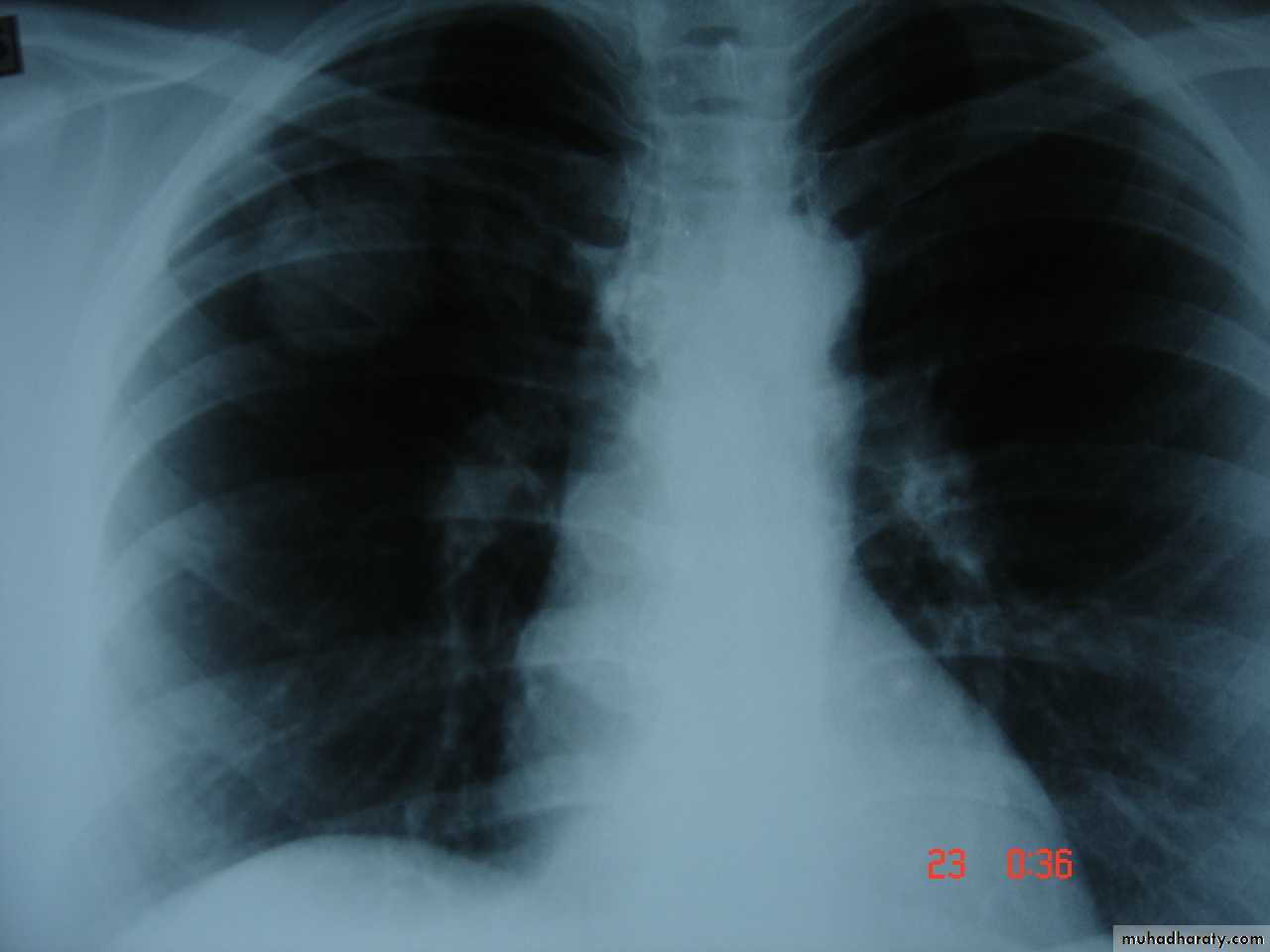
Bronchogenic Ca. cavitory lesion
• Pathology :-A-Central type is the commonest (75%).It arises in one of the main bronchi or their primary division leading to bronchial obstruction with secondary changes in the lung such as atelectasis .B-Peripheral type (25%) arises from the smaller bronchi and remains symptom less for long time .



Histologically Squamous cell Ca (SCC) 60% , smoker , centrally located ,metastasizes to mediastinal & supraclavicular LN . Adenocarcinoma (15% ) , located peripherally , more in women .Tends to metastasizes to the liver , brain ,bone & adrenals in addition to the LN Undifferentiated carcinoma (oat) cell carcinoma and large cell carcino(20-30%) which includes small cell Ca Alveolar cell carcinoma , located peripherally ,metastasizes to the liver and adrenalsRecent classification..Non small & small cell carcinoma
• Superior sulcus tumor of Pancoast It is a low grade epidermoid carcinoma that grows slowly and metastasize late, infiltrates and involves lower root of Brachial plexus, intercostal nerves , Cervical sympathetic nerves & eroding the upper ribs ,producing pain in the shoulder & Horner's syndrome .
• Clinical features :-1- cough dry or productive2-Haemoptysis3-Chest pain4-Dyspnea5-Pleural effusion6-Anorexia & loss of weight7-Clubbing of the fingers8-Hoarseness of the voice (recurrent LN)9-Dysphagia involvement of the esophagus10-Hormonal syndromes ..ectopic ACTH , ADH, hypercalcaemia ,carcinoid syndrome
• Diagnosis
• Clinical , sputum cytology
• Chest X-ray ,CT chest ..
• Bronchoscopy ,BAL ,bronchial brush &biopsy
• FNAC….or Trucut biopsy , pleural fluid aspiration & cytology
• Diagnostic Thoracoscopy & mediastinoscopy
• TNM classification for staging
• Signs of inoperability :-1-Bloody pleural effusion .positive for malignant cells2-Horner’s syndrome .3-Vocal cord paralysis4-Phrenic nerve palsy(elevated hemi diaphragm)5-SVC obstruction 6-Distant metastasis 7-If during surgery ,the tumor locally spreading or cannot be remover technically or fixed to the PA or to the heart ,it is technically irresectable


• Treatment 1-Surgery more than 50%of the patients have distant metastases at the time of diagnosis .50% Iresectable per operatively15-20 % resectability rate Surgery ..segmentecomy , lobectomy . pneumectomy
2-Radiotherapy
Pre operative or post operative
Chemo therapy vincristine or adriamycin
Bleomycin for malignant effusion
• Bronchiectasis
• Is a persistent abnormal dilatation of the bronchi generally beyond the sub segmental level , generally classified as three types cylindrical , varicose & saccular . The left lower lobe is more commonly involved then the right lower lobe .• Aetiology :-
• 1-Congenital causes (25%) 2-Acquired causes (75%)
• The acquired causes include air way infection (bact. Or viral)
• bronchial obstruction (F.B., neoplasm.,LN)
• It present in 40% of patients with chronic middle lobe infection (middle lobe syndrome) which involved impaired clearance of secretion mostly due to a pressure of enlarged LN.
• Congenital Bronchiectasis (Kartagner’s syndrome)
• It includes (Bronchiectasis , situs inversus ,sinusitis ,sperms hypo motility ) .It represents genetic disorder with abnormal ciliary motility so impaired clearance of sputum with the resultant bronchiectasis .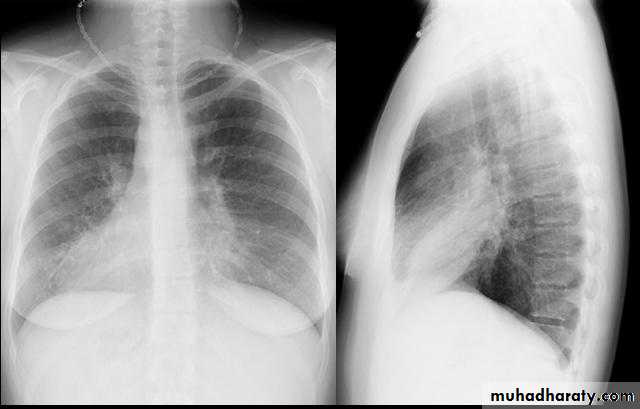
• Clinical manifestation :-The onset is mostly in childhood whereas symptoms generally appear in the second or third decade of life .The disease is more common in females .Major symptom cough with the production of purulent sputum with fetor oris .50% of the patients presented with haemoptysis .Others present with repeated RT infection .,others develop osteo arthropathy & finger clubbing which will resolve with treatment .
• Diagnosis :-
• 1-History chronic cough with purulent sputum.
• 2-Plain CXR may shows prominent vascular marking .
• 3-Bronchoscopy to diagnose obstructive lesion & to obtain bronchial wash for C&S test .
• 4-Bronchography through giving radio opaque dye through the bronchoscope & into bronchial tree ,now replaced completely by CT.
• 5-Chest CT is the single non invasive tool for both diagnosing &assessing the severity of the disease .
• 6-X-Ray paranasl sinuses to treat any excisting infection .
• 7-Pulmonary function tests very important specially in pre operative assessment .
• Treatment :-
• Medical treatment is the main stay of treatment ,it includes antibiotics , chest physiotherapy &postural drainage .• Surgical treatment in cases of failure of medical treatment and it includes segmentectomy , lobectomy & pneumonectomy