OSTEOCHONDRITIS (OSTEOCHONDROSIS)
Sadeq Al-Mukhtar Prof.Dr.Definition
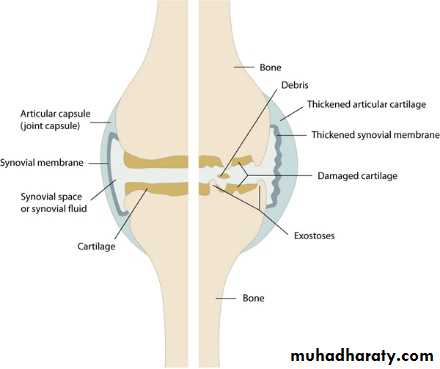
A group of conditions in which there is compression, fragmentation or separation of a small segment of articular cartilage and bone. The affected area shows many features of ischemic necrosis which include:-
Death of bone cells in the separated fragment and reactive vascularity
and osteogenesis in the surrounding bone.
ETIOLOGY
The causes have not been agreed upon, may be due to Vascular disturbance, possibly following trauma-impact injuries may cause bleeding or edema in the subarticular bone, resulting in capillary compression or thrombosis and localized ischemia.Traumatic factor
Traumatic factor is supported by frequent history of injury, by the greater frequency of the condition in boys, and by the more usual location either in weight- bearing joints such as the hip or in the epiphyses that are subjected to great strain.
Genetic factors may play a role
The relationship between osteochondritis and skeletal growth
It appears clinicallysoon after the appearance of ossification, e.g Perthes disease at four years and Osgood-Schlatter disease at eleven years;
during or immediately after the mid growth, or adolescent spurt e.g., Scheuermanns disease which is aggravated by adolescent growth spurt; and
earlier in girls than in boys because the later are slower in maturation.
Clinical manifestations
Bilateral or unilateral, the onset is usually gradual in a patient with good health who may offer a history of trauma. The symptoms include slight pain, limp in a weight-bearing joint, limitation of the movement, and at times muscle spasm. The symptoms are usually mild. Many cases are asymptomatic and discovered only when deformities develop.
Radiological findings
The radiological finding appearance is usually much more severe than the clinical picture .There is early osteoporosis with subsequent sign of repair. The epiphysis becomes fissured, fragmented broadened , and irregular in outline. Area of dense necrotic bone become evident. The process may involve the epiphysis and metaphysis. Later on replacement of the necrotic bone by new bone.

Types of osteochondritis
Crushing; Usually seen in late adolescence, but adults also are sometimes affected. It is characterized by apparently spontaneous necrosis of the ossific nucleus in a long-bone epiphysis or one of the cuboidal bones of the wrist or foot. Pain and limitation of movement are the usual complaints. Tenderness is sharply localized to the affected bone. X-Rays show the characteristic increased density , later on distortion and collapse of the necrotic segmentExamples
Freibergs disease of the metatarsal.
Kohlers disease of the navicular.
Kienbocks disease of of the carpal lunate.
Panners disease of the capitulum.
Vertebral osteochondritis( Scheuermanns disease), which may cause back pain and dorsal kyphosis.
Splitting Osteochondritis
A small segment of articular cartilage and the subjacent bone may separate as an avascular fragment. This occur typically in young adult , usually men , and affect particular sites; the lateral surface of the medial femoral condyle in the knee, the anteromedial corner of talus in the ankle. The superomedial part of the femoral head, the humeral capitulum and the first metatarsal head.The cause is almost certainly repeated minor trauma resulting in osteochondral fracture, the fragment loses its blood supply.
The knee is much the commonest joint to be affected. The patient presents with intermittent pain, swelling and joint The detached fragment may cause locking of the joint, and effusion
TREATMENT
In early stage consists of load reduction and restriction of activity.
In children, healing may occur, it may take 2 years.
In adult the treatment depend on its size and degree of detachment.
Pulling Osteochondritis
Localized pain and increased radiographic density in an unfused apophysis may result from tensile stress on the physeal junction. This is seen in two sites ;the tibial tuberosity( osgood-schlatters disease) and the calcaneal apophysis( severs disease). This is due to unusual traction forces from powerful tendons which insert into the apophysis . The bony changes here never leads to true necrosis.
THANK YOU