Cestodes (tapeworms)
Subjects to be discussedTypes of cestodes
Life cycles
Clinical presentation
Investigation
Treatment
Introduction:
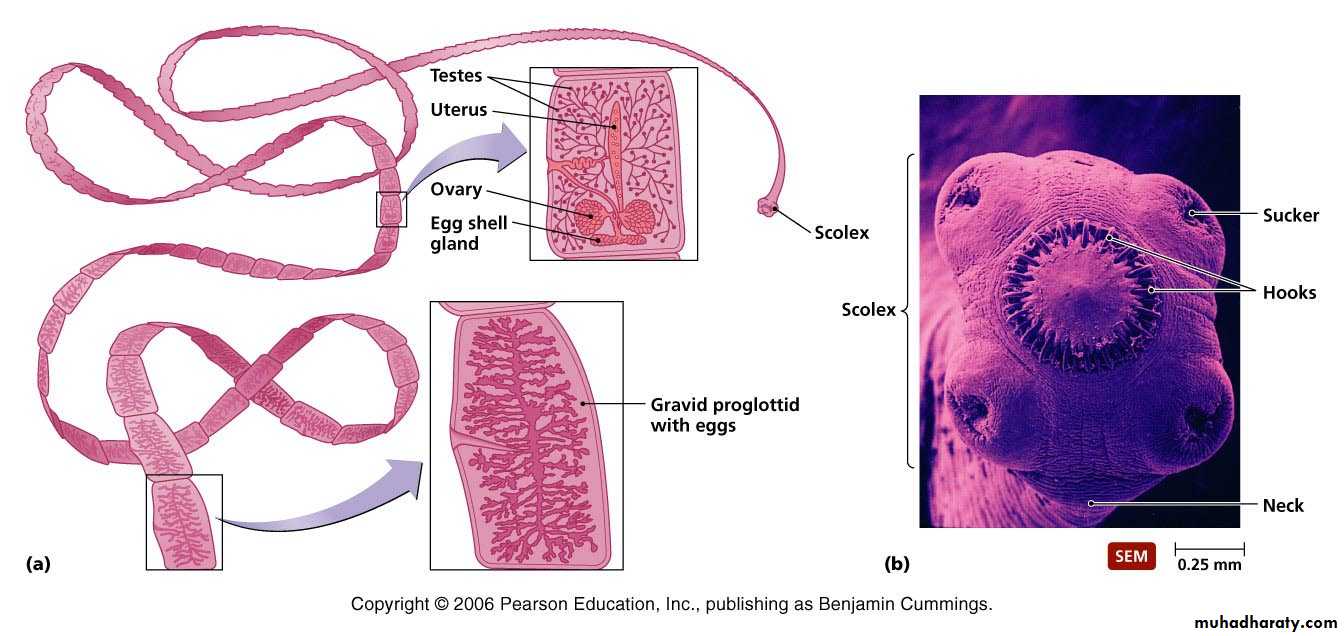
Cestodes are ribbon-shaped worms which inhabit the intestinal tract. They have no alimentary system and absorb nutrients through the tegumental surface. The anterior end, or scolex, has suckers for attaching to the host. From the scolex arises a series of progressively developing segments, the proglottides, which, when shed, may continue to show active movements.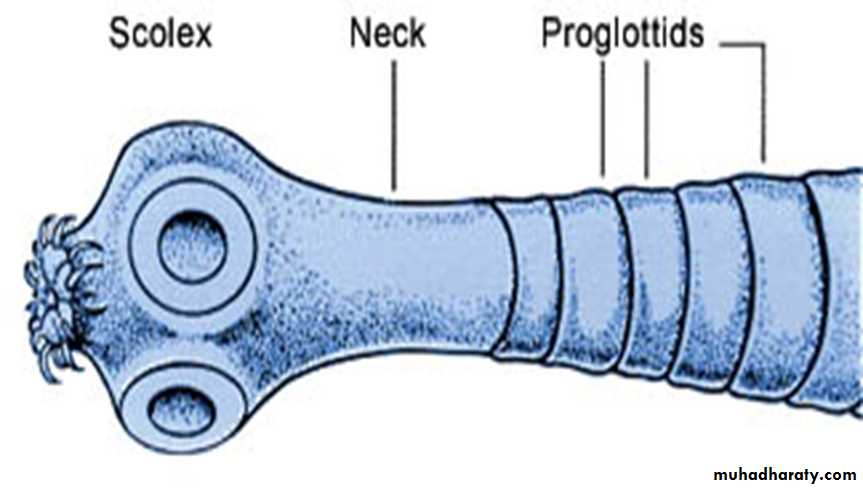
Adult Tape Worm
Cross-fertilisation takes place between segments. Ova, present in large numbers in mature proglottides, remain viable for weeks and during this period they may be consumed by the intermediate host.
Larvae liberated from the ingested ova pass into the tissues, forming larval cysticerci.
Cestodes or tapeworms include:
Intestinal tapeworms: Taenia saginata, T. solium, Diphyllobothrium latum, Hymenolepis nana.Tissue-dwelling cysts or worms: Taenia solium, Echinococcus granulosus .
Tapeworms cause two distinct patterns of disease:intestinal infection
systemic cysticercosis.
Taenia saginata (beef tapeworm) and Diphyllobothrium latum (fish tapeworm) cause only intestinal infection, following human ingestion of intermediate hosts that contain cysticerci (the larval stage of the tapeworm).
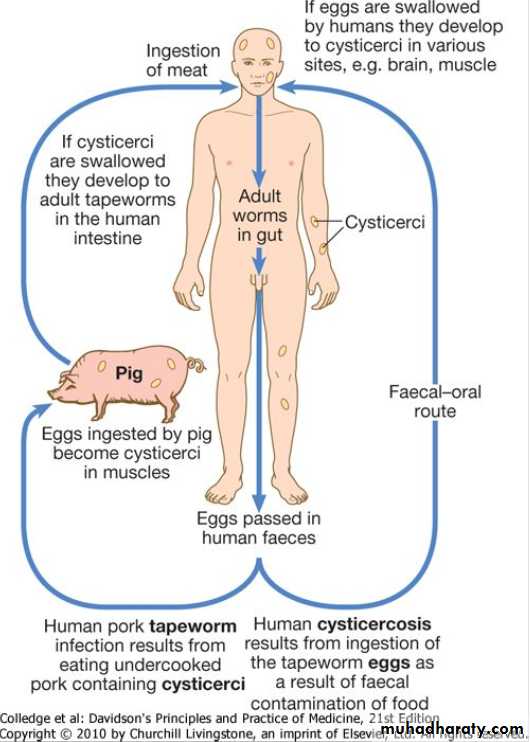
Taenia solium causes intestinal infection if a cysticerci-containing intermediate host is ingested, and cysticercosis (systemic infection from larval migration) if ova are ingested.
Echinococcus granulosus (dog tapeworm) does not cause human intestinal infection, but causes hydatid disease (which is analogous to cysticercosis) following ingestion of ova and subsequent larval migration.
Intestinal tapeworm
Humans acquire tapeworm by eating undercooked beef infected with the larval stage of T. saginata or undercooked pork containing the larval stage of T. solium.Usually only one adult tapeworm is present in the gut but up to ten have been reported.
Taenia saginata
Infection with T. saginata occurs in all parts of the world. The adult worm may be several metres long and produces little or no intestinal upset in human beings, but knowledge of its presence, by noting segments in the faeces or on underclothing, may distress the patient. Ova may be found in the stool. Praziquantel is the drug of choice. Prevention depends on efficient meat inspection and the thorough cooking of beef.
Taenia solium
T. solium, the pork tapeworm, is common in central Europe, South Africa, South America and parts of Asia. It is not as large as T. saginata. The adult worm is found only in humans following the eating of undercooked pork containing cysticerci. Niclosamide, followed by a mild laxative (after 1-2 hours) to prevent retrograde intestinal autoinfection, is effective for intestinal infection. Cooking pork well prevents intestinal infection.Cysticercosis
Human cysticercosis is acquired by ingesting T. solium tapeworm ova, from either contaminated fingers or food . The larvae are liberated from eggs in the stomach, penetrate the intestinal mucosa and are carried to many parts of the body where they develop and form cysticerci, 0.5-1 cm cysts that contain the head of a young worm. They do not grow further or migrate. Common locations are the subcutaneous tissue, skeletal muscles and brain.
Life cycle of the pork tapeworm
Clinical features
When superficially placed, cysts can be palpated under the skin or mucosa as pea-like ovoid bodies. Here they cause few or no symptoms, and will eventually die and become calcified.Heavy brain infections, especially in children, may cause features of encephalitis. More commonly, however, cerebral signs do not occur until the larvae die, 5-20 years later. Epilepsy, personality changes, staggering gait or signs of internal hydrocephalus are the most common features.
Investigations
•Calcified cysts in muscles can be recognised radiologically. In the brain, however, less calcification takes place and larvae are only occasionally visible by plain X-ray; usually CT or MRI will show them. Epileptic fits starting in adult life suggest the possibility of cysticercosis if the patient has lived in or travelled to an endemic area. The subcutaneous tissue should be palpated and any nodule excised for histology. Radiological examination of the skeletal muscles may be helpful.•Antibody detection is available for serodiagnosis.
Management and prevention
• Albendazole, 15 mg/kg daily for a minimum of 8 days, has now become the drug of choice for parenchymal neurocysticercosis.
• Praziquantel is another option, given daily for 10 days.
• Prednisolone, is also given for 14 days, starting 1 day before the albendazole or praziquantel.
In addition, anti-epileptic drugs should be given until the reaction in the brain has subsided.
Echinococcus granulosus (Taenia echinococcus) and hydatid disease
Dogs are the definitive hosts of the tiny tapeworm E. granulosus. The larval stage, a hydatid cyst, normally occurs in sheep, cattle, camels and other animals that are infected from contaminated water. By handling a dog or drinking contaminated water, humans may ingest eggs. The embryo is liberated from the ovum in the small intestine and gains access to the blood stream and thus to the liver.The resultant cyst grows very slowly, sometimes intermittently. It is composed of an enveloping fibrous pericyst, laminated hyaline membrane (ectocyst) and inner germinal layers (endocyst) which gives rise to daughter cysts, or germinating cystic brood capsule in which larvae (protoscolices) develop.
Over time some cysts may calcify and become non-viable.
The disease is common in the Middle East, North and East Africa, Australia and Argentina. E. multilocularis, which has a cycle between foxes and voles, causes a similar but more severe infection, 'alveolar hydatid disease', which invades the liver like cancer.
Clinical features
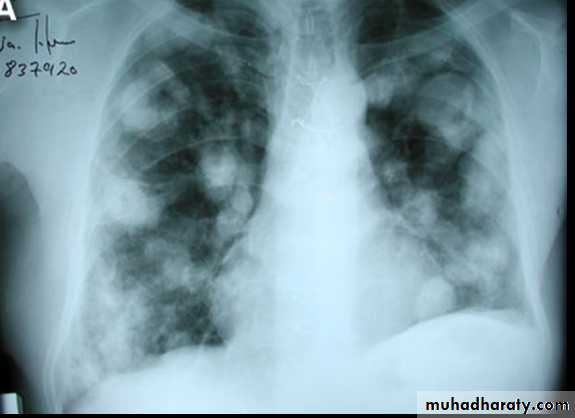
A hydatid cyst is typically acquired in childhood and may after growing for some years, cause pressure symptoms. These vary, depending on the organ or tissue involved. In nearly 75% of patients with hydatid disease the right lobe of the liver is invaded and contains a single cyst. In others a cyst may be found in lung, bone, brain or elsewhereLife cycle of Echinococcus granulosus
Daughter cysts removed at surgeryInvestigations
The diagnosis depends on the clinical, radiological and ultrasound findings in a patient who has lived in close contact with dogs in an endemic area. Complement fixation and ELISA are positive in 70-90% of patients.
Abdominal CT Scan show. Large hepatic hydatid cyst

Brain MRI show. LF frontal lobe H.cyst

CXR With multiple H.cysts
Management and prevention
Hydatid cysts should be excised wherever possible. Great care is taken to avoid spillage and cavities are sterilised with 0.5% silver nitrate or 2.7% sodium chloride.Albendazole (400 mg 12-hourly for 3 months) should also be used. The drug is now often combined with PAIR (percutaneous puncture, aspiration, injection of scolicidal agent and re-aspiration) to good effect.
Praziquantel for 14 days also kills protoscolices perioperatively.
Prevention is difficult in situations where there is a close association with dogs and sheep. Personal hygiene, satisfactory disposal of carcasses, meat inspection and deworming of dogs can greatly reduce the prevalence of disease.
Thank You